
By Charly D. Miller,
Paramedic EMS Author & Educator,
Consultant Restraint Asphyxia Expert Witness
Updated (finally!) in SEPTEMBER, 2004
PLEASE NOTE: If by some Internet fluke you've reached this page without first having read
Restraint Asphyxia – Silent Killer, PART ONE, CLICK HERE NOW!

The "webpage" versions of "RASK" Parts 1 & 2 remain posted on this website.
Restraint Asphyxia – Silent Killer Parts 1 & 2 and References
However, in December, 2005, I created and posted a PDF file containing
BOTH Parts 1 & 2 of RASK, and
the REFERENCES for all the RASK article parts!
If you're going to PRINT these parts, I strongly suggest you print their PDF file:
AS discussed in Part One of this article: Restraint asphyxia researchers have been warning Restrainers about the lethal dangers of employing prone-hogtie or forceful-prone-restraint since the late 1980's.(1,3,11,12,16,17,20)
 In recent years, however, restraint asphyxia researchers have come to the relatively-universal agreement that:
In recent years, however, restraint asphyxia researchers have come to the relatively-universal agreement that:
RESTRAINT – by itself – is not solely responsible for the asphyxia that occurs while a Victim is being actively restrained by others.(1,4,5,12,17,18,21-25)
In fact, restraint asphyxia ONLY occurs when an asphyxiating form of restraint is preceded by and associated with certain very specific, lethally-exhausting and body-chemical-unbalancing, Victim-Activities.
However. The lethally-exhausting and body-chemical-unbalancing Victim-activities preceding and associated with restraint application – by themselves – do NOT cause death, either.(26,27,28)
THUS, in RESPONSE to these lethally-exhausting and body-chemical-unbalancing Victim-activities, IF the manner of restraint that is employed interferes with the Victim's ability to BREATHE, the asphyxiating form of restraint employed REMAINS the ultimate "cause" of the Victim's death.
To systematically describe and thoroughly explain how they place a Victim at risk for restraint asphyxia, I've separated these lethally-exhausting and body-chemical-unbalancing activities into 3 ACTIVITY "PHASES" – phases that have consistently been associated with EVERY recognized restraint asphyxia death ever documented.
Please read about these phases in order, beginning with PHASE 1 (immediately below this). However, to help those who make more than one "trip" here to read the article ONLINE, here are "skip to" links:
 |
 |
"Altered Level Of Consciousness" ONSET PHASE |
|
 |
PHASE 1 begins when an individual suddenly develops an "altered level of consciousness" that just happens to adversely effect the part of their brain that triggers them to involuntarily act-out in an unusually aggressive or violent, emotionally- and physically-exertive manner. Because it is caused by an altered level of consciousness (a state of "delirium") that produces violently "excited" or "agitated" behaviors, medical professionals call this state of extremely emotionally- and physically-exertive behavior, "AGITATED DELIRIUM" or "EXCITED DELIRIUM."
In simpler terms: some or all of the Victim's brain becomes "tweaked" by something. And, a PART of his brain that accidentally becomes seriously-tweaked begins ORDERING the Victim to act-out in an unusually aggressive or violent behavior.
Thus, the altered level of consciousness Victim is entirely incapable of volitionally "refusing" to respond to the ORDERS being issued by his tweaked-brain.
Anything that can cause someone to suffer an altered level of consciousness –
Anything that can "tweak" ANY part of someone's brain –
ALSO can "tweak" the part of the brain that triggers the INVOLUNTARILY
performance of unusually aggressive or violent behaviors.
The mnemonic, "AEIOU TIPS," serves to remind medical professionals of the many, many different emergencies or conditions that can cause someone to suffer an Altered Level of Consciousness:
A .. Acidosis (a body-chemistry imbalance) .. Alcohol intoxication
E .. Epilepsy (seizures ... "convulsions")
I .. Infection (especially when accompanied by fever)
O .. Overdose (of "medications," or "drugs," or alcohol)
U .. Uremia (a body-chemistry disorder)
T .. Trauma (to the head) ... Tumor (of the brain)
I .. "Insulin" (states of low or high blood sugar in diabetics or non-diabetics)
P .. Poisoning ... Psychosis (sudden onset)
S .. "Stroke" (TIA or CVA)Altered-Level-of-Consciousness Causes NOT Clearly Indicated
by the "AEIOU TIPS" Mnemonic:
- Unusual and unexpected adverse reactions to non-overdose-levels of ANY medication or drug ("idiosyncratic reactions" to ANY medication or drug) ...
- ANY OTHER "body-chemistry imbalance" causes; such as "water-intoxication" ... deficiency or overdose of ANY "electrolyte" or "vitamin" (potassium, calcium, magnesium, and so on) ...
- Sleep deprivation ...
- Sudden onset of a "manic" phase in an individual with a "bipolar" brain disorder ...
- Abrupt withdrawal from a prescribed medication that requires "weaning" to safely discontinue ...
- Essentially, the list of these causes is almost ENDLESS!
Obviously, it is vitally important for all Medical-Responders to understand the myriad of altered level of consciousness causes. But, why is it important for Non-Medical-Responders to understand them?
No matter where or for whom we work, we ALL are human beings. And, no matter how much "job experience" we have, we ALL involuntarily experience strong emotional responses, triggered by our personal interpretations of (our "gut reactions" to) EVERY "emergency" situation we face.
Thus, it is vitally important for ALL Restrainers to REMEMBER that:
In fact, almost ALL Restrainers are related to or personally acquainted with cherished individuals who have medical conditions (such as epilepsy or diabetes) that put them at greater risk than others for becoming an agitated delirium Victim!
And, ANY individual who – under "normal" circumstances – is a perfectly pleasant and respectable person, may suddenly become the Victim of an emergency that triggers an altered level of consciousness and induces a state of agitated delirium.
So, when we don't "know" the Victim, it is especially inappropriate for us to automatically assume that he is a drug or alcohol abuser, simply because he is acting-out in an aggressive or violent manner and "refusing" to follow our cues!
Because it is so vitally important to ALL Restrainers' attitudes that we remember the fact that violently-aggressive states of agitated delirium are involuntarily triggered by so many different tweaked-brain causes, I have decided to coin a BRAND NEW ABBREVIATION within this article's September 2004 update:
This new abbreviation does NOT need to become universally-accepted or used elsewhere.
I am using it only so that every time YOU (my reader) see the abbreviation, "T-BIA" ("TEE-bee-ah") you will be REMINDED that
Time Frames Related to PHASE 1
Most causes of T-BIA – such as head injury, acute psychotic or manic episodes, strokes, intoxication, and the like – require 30 minutes to an hour (sometimes even longer) before the Victim's exertive behavior causes him to become severely physically exhausted, and extremely susceptible to restraint asphyxia.
However, two T-BIA causes produce SEVERE states of physical exhaustion QUITE QUICKLY.
Full-Body Seizure Activity – all by itself – represents significantly-extreme total-body physical exertion condensed into a very brief period of time (merely three to five minutes!), producing "prominent oxygen desaturations" (potentially lethal states of oxygen depravation), and rapidly causing extreme physical exhaustion.(29,30)
A full-body seizure is caused by an "electrical storm" in the brain that makes every muscle in the Victim's body rapidly and forcefully contract and relax, in a manner that is faster and more forceful than any consciously-controlled muscular activity. EVERY muscle in the Victim's body!
During a full-body seizure, even the body's "sphincters" (the little muscular rings responsible for things like keeping urine inside the bladder and feces inside the bowel) are rapidly and forcefully contracted and relaxed. Which means that, they aren't "working well" during the seizure. Thus, during full-body seizures, Victims almost always loose control of their bladder, and often loose control of their bowel.
Furthermore, while the diaphragm is "seizing" it is not traveling into and out of the abdomen in a manner that effectively changes the air pressure inside the Victim's lungs. Thus, the Victim isn't breathing in any meaningful manner during the seizure, and his brain rapidly becomes starved for oxygen.(29,30)
Thankfully, once full-body seizures stop, MOST Victims are simply profoundly exhausted and confused. Most full-body seizure Victims simply require a few minutes to breathe and rest before their brain becomes able to function better.
BUT! If a seizure's "electrical storm" happens to tweak the part of the Victim's brain that triggers involuntary physically-exertive activity, and physically-exertive activity continues AFTER the seizure has stopped, the extreme physical exhaustion caused during the seizure becomes worsened, and the post-seizure T-BIA Victim rapidly becomes lethally exhausted.
Victims of a Sudden Onset of Hypoglycemia (Low Blood Sugar) also require very little time to suffer extreme physical exhaustion – whether or not their low blood sugar emergency is caused by a "diabetic" disorder. For instance: impressively healthy marathon runners who fail to adequately "carb-up" prior to a race will rapidly succumb to hypoglycemia, and fail to complete the race.
The brain is significantly sensitive to low blood sugar levels. In fact, the very FIRST "SIGN" of low-blood-sugar exhibited by a hypoglycemia Victim (whether or not he is a "diabetic") is an "altered level of consciousness," demonstrated by confusion or "abnormal" behavior.
Hypoglycemia also increases the brain's susceptibility to suffering damage due to "hypoxia" – a lack of adequate oxygen in the blood.(31-36) Thus, low blood sugar can also cause confusion or "abnormal" behavior due to the brain's inability to adequately obtain oxygen.
Additionally, because blood sugar is the vital form of "energy" required to fuel the body's mechanical (muscular) activity, a low blood sugar state – all by itself – rapidly produces profound physical exhaustion. After all, if adequate fuel is not available, but the muscles are forcefully-activated anyway, the muscles almost immediately become "exhausted."
Finally, the altered level of consciousness caused by a low-blood-sugar-brain-tweak often causes the Victim to act-out in a physically-exertive manner. Thus, just as fatiguing physical exercise can cause otherwise healthy and non-diabetic persons to suffer from low blood sugar(37,38), hypoglycemic events that cause a Victim to act-out in a physically-exertive manner can rapidly cause lethally-extreme physical exhaustion.(39,40)
PHASE 1 SUMMARY:
If a full-body seizure or low blood sugar is responsible for the Victim's PHASE 1 "Altered Level Of Consciousness Onset," and a T-BIA response is triggered, the Victim may become extremely physically exhausted within as few as 3 to 5 minutes after the ONSET of PHASE 1.
No matter WHAT kind of emergency condition causes the Victim's PHASE 1 "Altered Level Of Consciousness Onset" T-BIA response, the Victim is being involuntarily-cued to act-out in an unusually aggressive or violent, emotionally- and physically-exertive manner. The Victim is entirely unable to consciously control his behavior, and entirely unable to volitionally respond to verbal counsel or de-escalation techniques.
The MOMENT it starts, the T-BIA Victim's PHASE 1 emotionally- and physically-exertive behavior begins to physically exhaust ALL of the muscles in his body. His unusually aggressive or violent behavior presents a "threat" to the safety of himself or others. AND, the Victim requires some form of physical restraint.
PHASE 1's physically-exertive-activity continues until the individual's "out of control" T-BIA behavior
is noticed by someone who either
(A) begins some form of "intervention" (without training or authority); OR
(B) notifies those legitimately responsible for "intervening" with the Victim's behavior,
and the appropriate Responders arrive.
When Responders arrive they rapidly recognize that the Victim's altered level of consciousness makes verbal forms of "restraint" (the "least restrictive" forms of restraint) entirely ineffective. Thus, PHASE 2 begins the moment Responders act to physically INTERVENE with the T-BIA Victim's behavior.
During PHASE 2, the T-BIA Victim's excessively-exertive activity continues during his involuntary struggle with Restrainers. The physical exhaustion suffered by the Victim during PHASE 1 is increased (worsened) by the physical exhaustion suffered during his PHASE 2 struggle with Restrainers.
Time Frames Related to PHASE 2
Commonly, PHASE 2 is quite BRIEF. The moment Responders begin to employ "normally-effective," minimally-restrictive, techniques of hands-on restraint, they immediately discover that the T-BIA Victim is INCREDIBLY STRONG! In fact, Restrainers almost immediately realize that minimal-to-moderate amounts of force, minimal-to-moderate amounts of restraint, are entirely unable to safely or effectively "contain" the individual's movements.
Contrary to the assumption commonly made by many medically-educated individuals; the incredible strength exhibited by ALL T-BIA Victims is NOT due to "adrenalin" stimulation.
So? WHY are T-BIA Victims so STRONG?
A person's ability to perform feats of "strength" is entirely based upon his ability to tolerate PAIN. When someone is bench-pressing a barbell loaded with steel weights, it is only when it "hurts" too much to "push" additional weight that the person reaches his bench-press weight limit. If he continues his weight-lifting regimen, his muscles become better and better developed, allowing him to push more and more weight before it starts to HURT to much, and he has to stop.
When a person doesn't perceive PAIN STIMULUS in a "normal" manner:
When forcefully-restrained by others, a T-BIA Victim (or PCP-abuser) actually may exert so much resistance-force and "strength" that he fractures his own bones!
PHASE 2 SUMMARY:
PHASE 3 begins when an increasing number of Restrainers begin applying an increasing amount of restraint (and restraint force) – rapidly progressing to a maximum, "full-body," form of restraint.
(WHAT Makes The Effects Of These
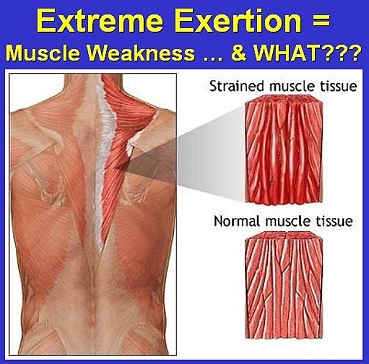
No matter what the original cause of the Victim's physically-exertive brain tweak, in addition to progressively exhausting all of the Victim's body muscles, each of the physically-exertive activity phases preceding and associated with restraint asphyxia cause INTERNAL CHEMISTRY IMBALANCES that adversely effect ALL of the individual's body functions.
Profound metabolic acidosis has consistently been noted in deaths "associated with cardiovascular collapse following exertion in a restrained position," and in other forms of asphyxial (suffocation) deaths.(26-28,41)
Two published scientific studies, performed under controlled clinical situations, have yielded information indicating that minimal-to-moderate forms of "full-body" prone restraint (even with a tiny bit of "weight" applied to the Victim's shoulders) do NOT produce obviously-lethal respiratory-interference effects in entirely-healthy study subjects.(21,49)
When a T-BIA Victim has suffered the adverse physical and chemical effects of one or more physically-exertive activity PHASES, and the manner of restraint employed to control him interferes – even minimally – with his ability to breathe, the Victim's need for oxygen progressively increases, but less and less oxygen is available.(1,17,26,41,50)
The moment a restrained Victim's respiratory bellows system is prevented from changing the internal air pressure within his lungs, the Victim can no longer breathe. Thus, the Victim suffers "RESPIRATORY ARREST" – even though HE IS STILL "CONSCIOUS" (AWAKE).
If diaphragmatic freedom to move (the ability to breathe) is not regained, a conscious respiratory arrest Victim rapidly becomes unconscious.(19) When one or more physically-exertive activity PHASES has preceded application of full-body-restraint that interferes with breathing,
Once unconscious, the respiratory arrest Victim's brain will instinctively and involuntarily cue his "accessory" muscles to continue to "struggle," in an effort to regain the ability to breathe.(19)
Unfortunately, the involuntary muscle movement of an unconscious respiratory arrest Victim does not stop until after the Victim's heart stops effectively circulating blood.(19)
The pathophysiology of death caused by purposefully-induced-asphyxia ("What happens to a body after it cannot breathe anymore?") has been clinically-studied in both dogs and rats.(19,41) "[Induced] Asphyxia led to cardiac arrest within approximately 4 minutes in all rats."(41) Clearly, a human being might take that long, or longer, or less long to die after asphyxia occurs. But, the amount of time it takes for a human being's heart to stop after respiratory arrest occurs cannot be clinically explored by experiment! So, we must rely upon evaluation of case studies to determine a reasonable estimate of how long it takes asphyxia to cause a human's heart to stop beating.
Even when the Victim is in the care of ACLS-providers who immediately notice the cardiopulmonary arrest, and immediately begin basic and advanced resuscitation measures, the Victim is not resuscitated.(20)
The currently-popular scientific theories offered to explain this failure-to-resuscitate phenomenon revolve solely around the fact that:
OR click on the following link to a PDF file of that information:
Current research suggests that rapidly-administered "aggressive ventilation and bicarbonate therapy" offers restraint asphyxia Victims the best possible chance of survival.(26,41) Deep and rapid artificial ventilation ("aggressive" hyperventilation) has long been proven to reverse systemic acidosis caused by respiratory-failure.(42-48,57,58) But, because restraint asphyxia Victims also suffer from such unusually-extreme muscle-exertion lactic-acid-production (prior to suffering from "common" respiratory-failure acid-production), they require more than merely "aggressive" hyperventilation to reverse their systemic accumulation of acid.
However, this supine total-body-restraint technique will
PLZ NOTE: I have NOT updated Part Three yet!
About the Author: Charly is an internationally-known emergency care author, EMS Instructor, Consultant, and Restraint Asphyxia Expert Witness.
A paramedic since 1985 (nine years as a "Denver General" Paramedic), Charly is a seasoned prehospital emergency care provider. With his additional experience as a psychiatric medical technician and an Army National Guard helicopter medic, Charly is one of the country's most exciting and entertaining EMS educators.
![]()
Photo © 1997 Howard M. Paul
2
The
INTERVENTION-
INITIATION
PHASE
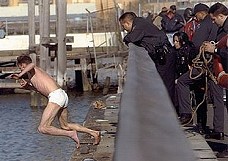
If initiated in an open space (out-of-doors), this phase often begins with a "chase." If Responders are law-enforcement, security, or correctional officers, the beginning of this phase is often accompanied by employment of things such as pepper spray, mace, Taser guns, or the like.
But, because the Victim is being involuntarily-cued to perform violent or aggressive exertional activity; no matter who the Responders are – no matter what initial setting or circumstances are involved – the Victim is involuntarily compelled to RESIST Restrainers' attempts to stop him from performing the violent or aggressive exertional activity.
Thus, this phase ALWAYS includes a period of "wrestling" (violent struggle) between Restrainers and the Victim.
If a maximum, "full-body," form of restraint that interferes with breathing (such as forceful-prone-restraint) is the first form of restraint applied by Responders, restraint asphyxia death can occur during PHASE 2.
PLZ NOTE: T-BIA Victims are rarely ever "Arnold-Schwarzenegger"-types! Most often, they are
"White-Bread-Eating-Couch-Potatoes." Essentially, what I mean by that terrifically flippant label is this:
T-BIA Victims usually are individuals with absolutely NO "weight-training" or "body-building" background.
Most often, T-BIA Victims are simply "regular people."
In fact, T-BIA Victims most frequently are overweight and "out of shape" people!
Yes. T-BIA Victims are experiencing adrenalin ("fight/flight" system) stimulation. But, adrenalin stimulation automatically makes people "go faster" ... it does NOT automatically make people "stronger.")
For some (still unclear) reason; when an altered-level-of-consciousness-cause happens to tweak the part of the brain that triggers a Victim to involuntarily act-out in a violent or agitated and exertive manner,
perceive PAIN STIMULUS in a "normal" manner!
"PCP" (phencyclidine) is a drug used to tranquilize large animals (horses, elephants, and the like). It is an "anesthetic" with "analgesic" properties – in other words, PCP eliminates PAIN perception. When a human being takes PCP, the drug does NOT make him "stronger." It makes him unable to perceive PAIN. And, THAT is why PCP-abusers are so incredibly "strong!"
STRENGTH that someone can exert is "STRUCTURAL" in nature.
AND, because the T-BIA Victim perceives NO PAIN – no matter how much he exerts his muscles – his ability to perform incredible feats of strength is limited only by things like bone-density and tendon-anchor-adherence-strength factors.
do NOT bother the person.
He may exert so much resistance-force and "strength" that he RIPS the tendons that anchor his muscles to his bones from their moorings!
Clearly, such injuries will immediately cause the T-BIA Victim's injured limb to WORK less effectively (and more easily be restrained). However, since the Victim feels no pain, the parts of his body that remain uninjured continue to struggle with tremendous strength.
PHASE 2 activity begins the moment Responders act to physically INTERVENE with the T-BIA Victim's behavior.
PHASE 2 is usually a BRIEF phase, because Restrainers rapidly realize that the T-BIA Victim is INCREDIBLY STRONG, and that minimal-to-moderate amounts of "normally-effective" restraint techniques are entirely unable to safely or effectively "contain" the individual's movements.
The physical exhaustion suffered by the Victim during PHASE 1 is increased (worsened) by the physical exhaustion suffered during PHASE 2 struggle with Restrainers.
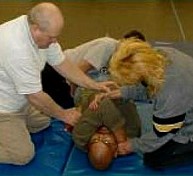
CONTINUED STRUGGLE
PHASE: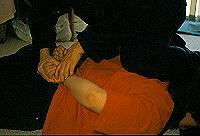
Photo © 1997 Howard M. Paul
The physical exhaustion suffered by the T-BIA Victim during PHASES 1 and 2 continues to be increased (worsened) by the physical exhaustion that occurs during the involuntary struggle against maximum restraint in PHASE 3. But, by now, the T-BIA Victim is ENTIRELY physically exhausted. Thus, if the manner of maximum "full-body" restraint employed prevents the Victim from being able to adequately breathe, respiratory arrest rapidly occurs.
The Exertional Phases of Activity
Preceding & Associated with
Restraint-Asphyxia
PHASES So LETHAL?!)
However, profound metabolic acidosis is not a finding associated with victims of a "common" cardiopulmonary arrest – a suddenly-occurring "heart attack," caused by heart disease or heart circulation problems.(26,42-48)
Thus, if the restraint asphyxia Victim is documented as being in a state of metabolic acidosis upon his emergency department arrival (especially in spite of rapidly-provided pre-hospital resuscitation measures), and no autopsy evidence clearly identifies another cause of his death; anyone who opines that his death was due to "cardiopulmonary arrest" does so without ANY form of scientific or forensic supportive evidence.
In fact, anyone who opines that the death of ANY victim with such a profound state of metabolic acidosis measured upon his arrival at the emergency department was solely due to "cardiopulmonary arrest," does so in spite of scientific and forensic evidence that the victim's death was much more likely due to some form of asphyxia.
As more and more sugar is used up by unusually-exertive muscular activity, less and less sugar is available to the muscles, causing all the body's muscles to become less-well fueled, more and more fatigued.(39,40) The more sugar that is used up to fuel unusually-exertive extremity muscular activity, the less sugar is available to the Victim's BRAIN – which means that his brain-tweak gets worse, and brain damage can occur!(31-36)
During all of the emotionally- and physically-exertive activities that precede and are associated with restraint asphyxia deaths, progressively-increasing amounts of catecholamines are released into the Victim's system. This creates what medical professionals call a, "hypercatabolic state" – an "overdose" of these naturally-produced chemicals.
A hypercatabolic state is a chemical imbalance that weakens ALL of the body's muscles. But, it especially weakens the respiratory muscles.(1,12)
So, because our respiratory muscles are entirely unaccustomed to exerting excessive effort to accomplish breathing, our respiratory muscles do not boast a significant amount of "muscle tone" or "strength." Thus, when faced with extreme-exertion requirements and body chemical imbalances, our respiratory muscles begin to "fail" long before our extremity muscles do.
Catecholamines cause the heart to contract (beat) faster, and with greater FORCE of contraction – exerting greater "effort" to work. Since the heart is a muscle that (like the respiratory muscles) is entirely unaccustomed to having to work terrifically hard for a prolonged period of time, the heart rapidly becomes exhausted when required to work harder than it is used to working.
Furthermore; to work FASTER and more FORCEFULLY, the heart muscle requires more SUGAR and OXYGEN to fuel an increased functional-performance demand.
But, when struggling against Restrainers, the Victim's extremity muscles are using up the vast majority of the body's sugar stores. So, less and less sugar is available to fuel the heart's function.
CONSIDERATIONS
However (again), the physically-exhausting and body-chemical-unbalancing effects caused by Victim-activities preceding and associated with restraint application – by themselves – do NOT cause death.(26,27,28)
The prolonged muscle-exertion lactic acidosis overdose can naturally be "hyperventilated" away ... once the cause of his delirium is corrected, the Victim's catecholamine overdose will naturally begin to dissipate (being filtered and excreted by the his liver and kidneys) ... and so on.
Furthermore, physical exhaustion ONLY EVER results in "respiratory arrest" when the Victim's respiratory muscle function (particularly his diaphragm function) is interfered with.
This is why restraint asphyxia researchers' agreement with the concept that "restraint" – by itself – is probably not solely responsible for the vast majority of restraint asphyxia deaths" is a "QUALIFIED" agreement!
little-to-NOTHING to do with "real life" restraint situations!(22,23)
FURTHERMORE, not a single scientific experiment or case study has ever been performed or published (or anecdotally distributed), identifying even ONE incident wherein the adverse physical and chemical effects of delirium-triggered physically-exertive activities have EVER – by themselves – resulted in someone's DEATH.
In fact, in ALL documented accounts of deaths associated with individuals suffering a state of "excited delirium": if the Victims didn't die due to physical trauma (caused by jumping off of a building, or the like) or chemical overdose (drug or alcohol "overdose") – causes of death clearly evidenced at autopsy – the Victims ultimately died ONLY because they were subjected to a body position or form of restraint that interfered with (or entirely prevented) their ability to BREATHE!
THE BOTTOM LINE: States of "Excited" or "Agitated Delirium" have NEVER, ever, been demonstrated to – by themselves – result in someone's death. Thus, anyone who opines that "Excited" or "Agitated Delirium" was the "cause" of someone's death, does so without ANY form of scientific or forensic support.

TO
THE
"MIX"
Individuals with "a large abdominal panniculus" (a medically-polite phrase meaning people who are overweight and have "a big belly") are at extreme risk for rapid onset of restraint asphyxia from prone positioning.(23,25,51)
"A large, bulbous abdomen (a beer belly) presents significant risks because it forces the contents of the abdomen upward within the abdominal cavity when the body is in a prone position. This puts pressure on the diaphragm, a critical muscle responsible for respiration, and restricts its movement. If the diaphragm cannot move properly, the person cannot breathe."(51)
In other words: Simply putting someone with a big belly in a prone position immediately "sandwiches" his abdominal contents between the ground and his spine. The bones of his pelvis prevent abdominal contents from shifting away from his chest. So, the only place for them to go is toward his chest. This pushes on the diaphragm and immediately interferes with his ability to change the internal-air-pressure of his lungs.
Putting someone with a big belly in a prone position causes SOME breathing interference, even without any force being applied to his posterior torso! If his shoulders and hips are held in place, breathing immediately becomes difficult.
And, remember; when faced with extreme-exertion requirements and body chemical imbalances, respiratory muscles begin to "fail" long before extremity muscles do. Once the diaphragm fails, the Victim's bellows system fails.
In spite of his "altered" level of consciousness, while the respiratory arrest Victim is still awake, he will employ every muscle he possibly can in order to escape the asphyxiating position and regain the ability to breathe. In fact, when a manner of restraint has started to interfere with or entirely prevent breathing, there is absolutely NO PERCEIVABLE DIFFERENCE between:
the muscular activity of someone consciously struggling to "escape restraint," and
the muscular activity of someone consciously struggling to "regain the ability to breathe."
A conscious respiratory arrest Victim will employ his shoulders and arms, his legs and hips, his "accessory" chest and abdominal muscles, all in an effort to give his exhausted diaphragm room to contract and move into his abdomen, so as to change the internal-lung air pressure and allow him to breathe again.
within less than 3 minutes
after an asphyxiating-form of restraint was applied
Accessory muscles most commonly include those of the neck, shoulders, and intercostal muscles (the muscles between the ribs). But, when being "trapped" or "restrained" in an asphyxiating position, arm and leg muscles may also be instinctively and involuntarily cued to move. Thus, several of the Victim's body muscles will continue to "move" after loss of consciousness – albeit in a less focused and forceful manner than that of consciously-controlled muscle movement.
Uneducated restrainers erroneously interpret this continued muscular activity as an indication that the individual is "still breathing" and/or still "fighting" with them. Consequently, restraint is continued.
In fact, restraint often is maintained until well after the Victim stops moving. When all movement stops, uneducated restrainers often assume that the restrained individual is "playing possum." Thus, they continue restraint application until they finally notice that the individual is no longer breathing ... is turning "blue" ... and/or has no pulse.
I assessed the times documented in several published restraint asphyxia case studies, to determine the average time interval between first application of forceful-prone-restraint and when Restrainers finally realized that the Victim was not breathing and did not have a pulse.(1,11,18, 20,52)
and when full cardiopulmonary arrest was noticed
is only 5.6 minutes!
– once his heart has finally stopped –
successful resuscitation is virtually unheard of.(20,25,26,41)the therapeutic effects of almost ALL medications administered during
At the time respiratory arrest occurs, the restraint asphyxia Victim already has a high systemic level of struggle-related lactic acidosis. Furthermore, both the conscious and unconscious muscle-exertion that is continued by the restraint asphyxia Victim, after respiratory arrest occurs, produces additional lactic acid.
standard Advanced Cardiac Life Support (ACLS) cardiopulmonary resuscitation
protocol-performances are interfered with ("inactivated")
if the Victim's internal body-system is chemically-imbalanced – especially if
the Victim has an excessively ACIDOTIC internal body-system.(26,41,53-56)
BUT, when respiratory arrest occurs and exchange of oxygen and carbon dioxide stops, ANOTHER cause of acid-production begins – an inadequate-ventilation form of acid production, that is called, "RESPIRATORY" acidosis.
Thus, the degree of acidosis measured in restraint asphyxia Victims is significantly greater than the degree of acidosis measured in Victims of a "common" cardiopulmonary arrest (a suddenly-occurring "heart attack" caused by heart or heart circulation problems).(26,41-47,57,58)
acidosis levels as they compare to restraint asphyxia acidosis levels,
Click Here to Go To That Webpage
Since Sodium Bicarbonate ("Bicarb") is considered the chemical "ANTIDOTE" to excessive levels of acidosis (whether from muscle-released lactic acidosis, or from respiratory-failure acidosis), researchers have hypothesized that rapid administration of Bicarb to restraint asphyxia Victims should correct their acidosis. AND, researchers have hypothesized that; once the asphyxia-victim's acidosis is corrected, standard ACLS medications should then work as effectively as they normally do for "common" cardiopulmonary arrest Victims' resuscitation.
Unfortunately, the clinical studies exploring these hypotheses, as well as case studies of restraint asphyxia victims who received Bicarb, have failed to demonstrate that rapid Bicarb administration is successful for effectively resuscitating extremely acidotic asphyxial cardiopulmonary arrest Victims.(26,27,41)
Thus, once a restraint asphyxia Victim's heart has finally stopped, successful resuscitation remains virtually unheard of.
accomplishing SUPINE total-body-restraint
in a manner that is every bit as immobilizing
as that of forceful-prone- or prone-hobble-restraint.
NOT threaten the patient's life with restraint asphyxia!
Photo © 1994 Michal Heron
I especially need to include discussion of using a
long back board for all patients requiring restraint and medical care.
Plus! For the 2004 Part Three Update, I'll also address
A Few PHYSICAL RESTRAINT Techniques Used by
NON-Medical Care Providers: Those Who Care for
Developmentally Disabled and Mentally Ill individuals.
of RESTRAINT ASPHYXIA – SILENT KILLER
of RESTRAINT ASPHYXIA – SILENT KILLER
How To Avoid Restraint Asphyxia
 Email Charly at: c-d-miller@neb.rr.com
Email Charly at: c-d-miller@neb.rr.com
Those are hyphens/dashes between the "c" and "d" and "miller"