Newz Flash!
As of October, 2010, Charly’s Email address has CHANGED!
 Due to the vast number of pages and documents posted on CharlyDMiller.com, only the
Due to the vast number of pages and documents posted on CharlyDMiller.com, only the
MAIN PAGES of this website will reflect her NEW EMAIL ADDRESS for – possibly – a rather long time!
Only after Chas finally manages to purchase a COMPUTER PROGRAM that will
search and replace the OLD Email address found on all these documents
will ALL the pages on this website provide her NEW EMAIL ADDRESS! LOL
 Email Charly at: chas@novelholiday.com
Email Charly at: chas@novelholiday.com

To fully understand the incredible importance of this collection, you
MUST READ the following explanation of how this directory came to be!
[On subsequent trips to this Collection’s Directory Click Here to SKIP to the articles.]
How This Directory Came To Be:
On February 6, 2006, I discovered that “Anesthesiologists” have performed and published LOADS of clinical studies consistently documenting the following FACTS:
As it happens, the February 2006 Anesthesiologists’ study that led me to find many of the other studies in this collection (when I researched its references), was one that demonstrated how
 prone positioning ALSO interferes with
prone positioning ALSO interferes with
the ability of the heart to CIRCULATE BLOOD!:
“We conclude that turning healthy patients prone produces a
clinically significant reduction in cardiac output.”
It was while researching the February 2006 Anesthesiologists study’s references that I discovered how Anesthesiologists (as well as Pulmonologists and a variety of surgeons) knew that prone positioning caused serious (“clinically significant”) respiratory interference long before Reay et al began investigating and writing about restraint-related positional asphyxia cases (1988).
The Anesthesia and Analgesia article I’ve obtained that MOST predates the earliest Reay et al articles about Restraint Asphyxia was published in 1974!
Smith RH. One solution to the problem of the prone position for surgical procedures.
Anesth Analg, 1974 Mar-Apr;53(2):221-4.
The 1974 Smith article references 2 earlier articles related to the “problems” of prone positioning.
Those articles are dated 1961 and 1964!

While reading THESE study articles, I also discovered another important fact!
Knowing the dangers associated with prone positioning, Anesthesiologists (and all Surgeons who required patients to be prone for a procedure) LONG AGO developed several support techniques and devices – even a special surgical table – specifically designed to allow abdominal freedom of movement so that breathing would NOT be impaired while the patient was placed prone for surgery!
 The “Jackson” Surgery Table
|
|
 The “Wilson Frame”
Click Here for LARGER PIX |
developed to allow FREEDOM of ABDOMINAL MOVEMENT during Prone Positioning for surgery mentioned in this collection of articles: |
|
 AN IMPORTANT NOTE!:
AN IMPORTANT NOTE!:
In every article that describes the PRONE position IMPROVING respiratory
ventilation or function, the study subjects were ALWAYS positioned in a manner
that PREVENTED ABDOMINAL COMPRESSION!
This makes tonz of sense! If the abdomen is allowed to hang freely below a prone body (the shoulders/chest and hips elevated, or the abdomen positioned over an open space), the diaphragm doesn’t have to “push” anything out of its way when it contracts and moves into the belly to produce inhalation. Additionally, gravity may assist the diaphragm’s descent, further lessening its work load and energy requirement, as well as increasing the amount of excursion (inhalation) that can be accomplished.
LESSON #1 Derived From This COLLECTION:
As discussed elsewhere on this website, employment of PRONE RESTRAINT by prehospital EMS personnel is CONTRAINDICATED for many more reasons than “only” that of impeding ventilation and asphyxiating someone to death! Thus, emergency RESTRAINT techniques will NEVER involve use of devices that assure “free abdominal movement” for a PRONE-restrained person.
BUT! These studies provide important “food for thought” when it comes to prehospital (or inhospital) care for victims of strange and bizarre situations that REQUIRE prone positioning during the patient’s emergency assessment, care and/or transportation.
For instance: situations involving an alert patient with a posteriorly-impaled object, or the like!
LESSON #2 Derived From This COLLECTION:
“Specialists” rarely ever research OTHER “Specialties” – and they SHOULD!
Anesthesiologists, Pulmonologists, Spine Surgeons (and the like) have been researching the effects of prone positioning for more than 30 YEARS! But, they had no idea that their prone position research was so important to the research being done by forensic pathologists (and other specialists) about prone restraint. So, they never thought to tell other specialists about it.
And, it never occurred to forensic pathologists (and others) who were researching restraint asphyxia issues to investigate other specialists’ studies for information related to the effects of prone restraint.
Thank goodness I finally stumbled upon these studies!
LESSON #3 Derived From This COLLECTION:
 The articles and studies in this collection clearly demonstrate
The articles and studies in this collection clearly demonstrate
the FACT that ALL the “CHAN ET AL” prone position study reports
& articles are ENTIRELY WITHOUT MERIT!!!
Unconscious, intubated and mechanically ventilated(!), human beings have LONG been shown to suffer serious respiratory compromise due to prone positioning’s interference with abdominal excursion.
Thus, there can be absolutely NO DOUBT that
FORCEFUL-PRONE-RESTRAINT applied to exhausted-yet-still-struggling
persons who are unintubated and NOT being ARTIFICIALLY VENTILATED,
DOES interfere with their abdominal excursion –
and DOES cause RESPIRATORY COMPROMISE!
‘Nuff said.
The Collection of Anesthesiology Studies follow the next few important messages.
| In early JUNE of 2009, charlydmiller.com Moved to a New Website HOST SERVER.
|
These Anesthesiology study reports are provided in PDF format.
You’ll have to use your BACK BUTTON to return to this directory page from any article.
So, be sure to BOOKMARK THIS PAGE before clicking on any of the article links.
That way, if you lose your Internet connection (for whatever reason)
while you read or print a file, you can easily GET BACK HERE.
If you don’t have an Adobe Acrobat PDF file program, you can download a FREE version HERE.
In April of 2008, 15 Prone Position & Ventilation Study Report CITATIONS were added
to this directory, in case they might be articles you are searching for. These studies are not
posted here. But their results are referred to (summarized) in
Sud S, Sud M, Friedrich JO, Adhikari NKJ.
Effect of mechanical ventilation in the prone position on clinical outcomes in patients with
acute hypoxemic respiratory failure: a systematic review and meta-analysis.
CMAJ Apr, 2008;178 (9); pgs 1153-1161.
As in the main Restraint Asphyxia Library article directory:
NAVY Text indicates a QUOTE from the linked article.
BLUE Text indicates a CHAS observation about the linked article.
PURPLE Text identifies when the abstract and/or article was posted on this site.
Effect of Mechanical Ventilation in the Prone Position on Clinical Outcomes
Prone position ventilation for community-acquired pneumonia [letter].
Reply to Friedrich et al [letter].
High-frequency oscillatory ventilation following prone positioning prevents a further impairment in oxygenation.
Inhaled nitric oxide and prone position: How far they can improve oxygenation in pediatric patients with acute respiratory distress syndrome?
Effects of prone position on inflammatory markers in patients with ARDS due to community-acquired pneumonia.
Haemodynamic Effects of the Prone Position: A Comparison
A multicenter trial of prolonged prone ventilation in severe acute respiratory distress syndrome.
Effect of prone positioning on clinical outcomes in children with acute lung injury: a randomized controlled trial.
Comparison of prone positioning and high-frequency oscillatory ventilation in patients with acute respiratory distress syndrome.
Prone positioning improves oxygenation in post-traumatic lung injury — a prospective randomized trial.
Effects of systematic prone positioning in hypoxemic acute respiratory failure: a randomized controlled trial.
Prone Position Improves Lung Mechanical Behavior and Enhances
Prone position effects on alveolar recruitment and arterial oxygenation in acute lung injury [abstract].
Prone position as prevention of lung injury in comatose patients: a prospective, randomized, controlled study.
Beneficial effect of a prone position for patients with hypoxemia after transthoracic esophagectomy.
Morbid Obesity and the Prone Position: A Case Report
Effect of prone positioning on the survival of patients with acute respiratory failure.
The Effect of Patient Positioning on Intraabdominal Pressure
The Effect of The Prone Position on Pulmonary Mechanics
Effects of the Prone Position on Respiratory Mechanics
Randomized trial compare prone vs supine position in patients with ARDS [abstract].
The Effects of Long-Term Prone Positioning in Patients With
Prone Positioning Improves Pulmonary Function
The Effect of Four Different Surgical Prone Positions on
The Prone Positioning During General Anesthesia Minimally Affects
One Solution to the Problem of the Prone Position for Surgical Procedures
Regarding the Effects of PRONE POSITIONING
in Patients With Acute Hypoxemic Respiratory Failure:
A Systematic Review and Meta-Analysis.
CITATION: Sud S, Sud M, Friedrich JO, Adhikari NKJ.
Effect of mechanical ventilation in the prone position on clinical outcomes in patients
with acute hypoxemic respiratory failure: a systematic review and meta-analysis.
CMAJ Apr, 2008;178 (9); pgs 1153-1161.
AND!!!
CITATION: Gattinoni L, Protti A.
Ventilation in the prone position: For some but not for all?
CMAJ Apr, 2008;178 (9); pgs 1174-1176.
CHAS NOTES:
This research review report (and its related Commentary article) is not related to the
effects of prone restraint application in the field, primarily because all the reviewed
studies’ subjects were intubated and being mechanically ventilated.
In Appendix 2 (pages 14-18 of this file), the authors identify the manner of prone
positioning employed for the studies “where reported.” Some subjects were in a
position where the abdomen was “unrestrained, using cushions to support abdomen
above bed surface.” Some subjects were in a position where the abdomen was
“restrained by direct contact with bed.” But, many of the studies did not report the
manner of prone positioning employed! [I cannot imagine WHY presumably
“intelligent” researchers would fail to consistently report such a vitally important
position-related ventilation factor.]
This file does, however, include SUMMARIES of the several prone-positioned
studies reviewed by these authors.
This article was originally posted in April of 2008.
By Friedrich JO, Sud S, Sud M, et al. J Formos Med Assoc 2008;107:191.
This letter is not posted here. Its content is referred to (summarized) in Sud S, Sud M, Friedrich JO, Adhikari NKJ. Effect of mechanical ventilation in the prone position on clinical outcomes in patients with acute hypoxemic respiratory failure: a systematic review and meta-analysis. CMAJ Apr, 2008;178 (9); pgs 1153-1161.
By Chan MC, Hsu JY, Liu HH, et al. J Formos Med Assoc 2008;107:192.
This letter is not posted here. Its content is referred to (summarized) in Sud S, Sud M, Friedrich JO, Adhikari NKJ. Effect of mechanical ventilation in the prone position on clinical outcomes in patients with acute hypoxemic respiratory failure: a systematic review and meta-analysis. CMAJ Apr, 2008;178 (9); pgs 1153-1161.
By Demory D, Michelet P, Arnal JM, et al. Crit Care Med 2007;35:106-11.
This study is not posted here. Its results are referred to (summarized) in Sud S, Sud M, Friedrich JO, Adhikari NKJ. Effect of mechanical ventilation in the prone position on clinical outcomes in patients with acute hypoxemic respiratory failure: a systematic review and meta-analysis. CMAJ Apr, 2008;178 (9); pgs 1153-1161.
By Ibrahim TS, El-Mohamady HS. Journal of Medical Sciences 2007;7:390-5.
This study is not posted here. Its results are referred to (summarized) in Sud S, Sud M, Friedrich JO, Adhikari NKJ. Effect of mechanical ventilation in the prone position on clinical outcomes in patients with acute hypoxemic respiratory failure: a systematic review and meta-analysis. CMAJ Apr, 2008;178 (9); pgs 1153-1161.
By Chan MC, Hsu JY, Liu HH, et al. J Formos Med Assoc 2007;106:708-16.
This study is not posted here. Its results are referred to (summarized) in Sud S, Sud M, Friedrich JO, Adhikari NKJ. Effect of mechanical ventilation in the prone position on clinical outcomes in patients with acute hypoxemic respiratory failure: a systematic review and meta-analysis. CMAJ Apr, 2008;178 (9); pgs 1153-1161.
of Propofol Total Intravenous and Inhalation Anaesthesia
CITATION: Sudheer PS, Logan SW, Ateleanu B, and Hall JE.
Haemodynamic effects of the prone position: a comparison of propofol total intravenous
and inhalation anaesthesia. Anaesthesia, 2006 Feb;61(2): 138–141.
[CHAS’ underlines] We conclude that turning healthy patients prone produces a
clinically significant reduction in cardiac output, … Measurements of non-invasive
blood pressure, heart rate and cardiac output were made in the supine position. The
patient was then turned prone onto a Montreal pattern mattress and measurements
repeated. … In University Hospital of Wales a preshaped Montreal pattern mattress is
the support used for prone patients, a widely used device. It is made of plastic coated
foam rubber with a central cavity to allow free movement of the abdomen and covered in
a full length jellypad to help distribute the pressure evenly. … The head and the lower
limbs are then slightly dependent with respect to the heart with the legs bent at the knee
over a bolster. The use of this frame has not been previously studied in the literature but
would be expected to perform similarly to the other devices (props) described in
Wadsworth et al.’s study [6]. … To conclude, our study suggests that when [healthy]
patients are turned into the prone position the cardiac index is reduced due to a reduction
in venous return and ventricular compliance, …
Plz NOTE: The “clinically significant reduction in cardiac output” suffered by these
prone-positioned patients occurred while they were on a support “with a central cavity
to allow free movement of the abdomen”! Imagine how much greater the cardiac output
reduction would have been, had the study subjects been prone-positioned with their
bellies compressed! Then imagine the even greater cardiac output reduction that
would have been suffered, had the study subjects been FORCEFULLY-prone-restrained!!!
This article was originally posted February 10, 2006.
By Mancebo J, Fernandez R, Blanch L, et al. Am J Respir Crit Care Med 2006;173:1233-9.
This study is not posted here. Its results are referred to (summarized) in Sud S, Sud M, Friedrich JO, Adhikari NKJ. Effect of mechanical ventilation in the prone position on clinical outcomes in patients with acute hypoxemic respiratory failure: a systematic review and meta-analysis. CMAJ Apr, 2008;178 (9); pgs 1153-1161.
By Curley MA, Hibberd PL, Fineman LD, et al. JAMA 2005;294:229-37.
This study is not posted here. Its results are referred to (summarized) in Sud S, Sud M, Friedrich JO, Adhikari NKJ. Effect of mechanical ventilation in the prone position on clinical outcomes in patients with acute hypoxemic respiratory failure: a systematic review and meta-analysis. CMAJ Apr, 2008;178 (9); pgs 1153-1161.
By Papazian L, Gainnier M, Marin V, et al. Crit Care Med 2005;33:2162-71.
This study is not posted here. Its results are referred to (summarized) in Sud S, Sud M, Friedrich JO, Adhikari NKJ. Effect of mechanical ventilation in the prone position on clinical outcomes in patients with acute hypoxemic respiratory failure: a systematic review and meta-analysis. CMAJ Apr, 2008;178 (9); pgs 1153-1161.
By Voggenreiter G, Aufmkolk M, Stiletto RJ, et al. J Trauma 2005;59:333-41. [discussion 341-343]
This study is not posted here. Its results are referred to (summarized) in Sud S, Sud M, Friedrich JO, Adhikari NKJ. Effect of mechanical ventilation in the prone position on clinical outcomes in patients with acute hypoxemic respiratory failure: a systematic review and meta-analysis. CMAJ Apr, 2008;178 (9); pgs 1153-1161.
By Guerin C, Gaillard S, Lemasson S, et al. JAMA 2004;292:2379-87.
This study is not posted here. Its results are referred to (summarized) in Sud S, Sud M, Friedrich JO, Adhikari NKJ. Effect of mechanical ventilation in the prone position on clinical outcomes in patients with acute hypoxemic respiratory failure: a systematic review and meta-analysis. CMAJ Apr, 2008;178 (9); pgs 1153-1161.
Gas Exchange Efficiency in Mechanically Ventilated
Chronic Obstructive Pulmonary Disease Patients
CITATION: Mentzelopoulos SD, Zakynthinos SG, Roussos C, Tzoufi MJ, Michalopoulos AS.
Prone position improves lung mechanical behavior and enhances gas exchange
efficiency in mechanically ventilated chronic obstructive pulmonary disease patients.
Anesth Analg. 2003 Jun;96(6):1756-67.
[CHAS’ underlines] We studied 10 moderate-to-severe COPD patients … [who were]
orotracheally intubated … [and] mechanically ventilated … because of acute respiratory
failure (ARF) … secondary to severe, acute bronchitis. … Anesthesia and
neuromuscular blockade were induced and maintained throughout the study period …
After pronation, abdominal movement-restriction was minimized(2). … Our
main findings were: … (c) in abdominal compression absence, posture change
(and especially pronation) does not affect hemodynamic status …
I’ve Emailed the lead author, asking for a description of how “abdominal movement-
restriction was minimized” for these study subjects. The (2) at the end of that statement
referenced a 1998 study article that is in this collection. That study report describes the
following as the study position they used: “In the prone position the head was
turned laterally and the arms were parallel to the body. A roll under the upper part of the
chest wall and a pillow under the pelvis were positioned in an effort to minimize restriction
of abdominal movements.”
Hopefully, I’ll someday be able to report THIS study’s means of prone positioning.
[As of July 26, 2006, I still haven’t heard from the lead author!]
This article was originally posted February 10, 2006.
By Gaillard S, Couder P, Urrea V, et al. Intensive Care Med 2003;29:S12.
This study is not posted here. Its results are referred to (summarized) in Sud S, Sud M, Friedrich JO, Adhikari NKJ. Effect of mechanical ventilation in the prone position on clinical outcomes in patients with acute hypoxemic respiratory failure: a systematic review and meta-analysis. CMAJ Apr, 2008;178 (9); pgs 1153-1161.
By Beuret P, Carton MJ, Nourdine K, et al. Intensive Care Med 2002;28:564-9.
This study is not posted here. Its results are referred to (summarized) in Sud S, Sud M, Friedrich JO, Adhikari NKJ. Effect of mechanical ventilation in the prone position on clinical outcomes in patients with acute hypoxemic respiratory failure: a systematic review and meta-analysis. CMAJ Apr, 2008;178 (9); pgs 1153-1161.
By Watanabe I, Fujihara H, Sato K, et al. Crit Care Med 2002;30:1799-802.
This study is not posted here. Its results are referred to (summarized) in Sud S, Sud M, Friedrich JO, Adhikari NKJ. Effect of mechanical ventilation in the prone position on clinical outcomes in patients with acute hypoxemic respiratory failure: a systematic review and meta-analysis. CMAJ Apr, 2008;178 (9); pgs 1153-1161.
CITATION: Brodsky JB, Oldroyd M, Winfield HN, Kozlowski PM.
Morbid obesity and the prone position: a case report. J Clin Anesth. 2001 Mar;13(2):138-40.
Thank you, E.V. of Seattle, for sending me (US) this article!
An improperly positioned prone patient can experience serious impairment of
cardiopulmonary function. However, with appropriate preparation, even an
extremely obese patient can safely tolerate the prone position. …
Twelve people were needed to turn her prone onto two conventional operating tables that
had been placed side by side. Extra large pelvic and shoulder bolsters were used (Figure 1).
Care was taken to position her over the bolsters to allow her abdomen to hang freely
(Figure 2). All pressure areas were padded.
This article’s abstract was originally posted February 10, 2006.
The actual article was posted July 26, 2006.
By Gattinoni L, Tognoni G, Pesenti A, et al. N Engl J Med 2001;345:568-73.
This study is not posted here. Its results are referred to (summarized) in Sud S, Sud M, Friedrich JO, Adhikari NKJ. Effect of mechanical ventilation in the prone position on clinical outcomes in patients with acute hypoxemic respiratory failure: a systematic review and meta-analysis. CMAJ Apr, 2008;178 (9); pgs 1153-1161.
and Blood Loss in Spinal Surgery
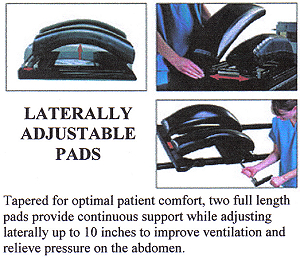
CITATION: Park CK. The effect of patient positioning on intraabdominal pressure and
blood loss in spinal surgery. Anesth Analg. 2000 Sep;91(3):552-7.
[CHAS’ underlines] Pressure on the abdominal contents [during prone-positioning is]
transmitted to the inferior vena cava, and then, to the epidural venous system, thus
causing increased bleeding [“during spinal surgery”](1). Any pressure on the anterior
abdominal wall causes vertebral venous pressure to increase. … The Wilson frame …
has two full-length pads which provide continuous support and adjust laterally to improve
ventilation and relieve pressure on the abdomen. However, if the pad width is too narrow
for the patient, the abdomen can be pressed and intraabdominal pressure (IAP) increases.
… In conclusion, [Intraabdominal Pressure] and intraoperative blood loss were
significantly less in the wide, than in the narrow, pad support width of the Wilson frame.
Blood loss tended to increase with an increase in IAP in the narrow pad support width of
the Wilson frame.
This article was originally posted February 10, 2006.
is Frame-Dependant
CITATION: Palmon SC, Kirsch JR, Depper JA, Toung TJK.
The effect of the prone position on pulmonary mechanics is frame-dependant.
Anesth Analg. 1998 Nov;87(5):1175-80.
[CHAS’ underlines] By compressing the abdomen and restricting chest wall movement, the
prone position compromises pulmonary compliance. For spine surgery, placing the
anesthetized patient into the prone position increases the risk of improper ventilation. …
In this study, we evaluated the three most popular [surgical frame] positioning devices at
our hospital. The chest rolls are placed longitudinally along the lateral torso from just
below the clavicle to the pelvis (Figure la). The Wilson frame is a curved frame that
supports the torso and pelvis along the lateral edges (Figure lb). The Jackson table has
padded supports under the chest and pelvis (Figure lc). These devices are intended to
elevate the anterior surface of the body so that the abdomen can hang freely and prevent
the abdominal viscera from impeding the inspiratory movement of the diaphragm.
… In this study, we demonstrated that prone positioning during anesthesia results in a
decrease in pulmonary compliance that is frame[device or table] -dependent but that is
not affected by body mass index.
This article was originally posted February 10, 2006.
and Gas Exchange During Acute Lung Injury
CITATION: Pelosi P, Tubiolo D, Mascheroni D, Vicardi P, Crotti S, Valenza F,
Gattinoni L. Effects of the prone position on respiratory mechanics and gas exchange during
acute lung injury. Am J Respir Crit Care Med. 1998 Feb;157(2):387-93.
[CHAS’ underlines] Thirteen patients were nasotracheally intubated with a cuffed
endotracheal tube ... and three had tracheostomies … All patients were studied while
sedated with fentanyl … and diazepam …, paralyzed with pancuronium bromide …, and
ventilated in the volume control mode with constant inspiratory flow.
… In the prone position the head was turned laterally and the arms were parallel to the
body. A roll under the upper part of the chest wall and a pillow under the pelvis were
positioned in an effort to minimize restriction of abdominal movements.
This article was originally posted February 10, 2006.
By Leal RP, Gonzalez R, Gaona C, et al. Am J Respir Crit Care Med 1997;155:A745.
This study is not posted here. Its results are referred to (summarized) in Sud S, Sud M, Friedrich JO, Adhikari NKJ. Effect of mechanical ventilation in the prone position on clinical outcomes in patients with acute hypoxemic respiratory failure: a systematic review and meta-analysis. CMAJ Apr, 2008;178 (9); pgs 1153-1161.
Trauma-Induced Adult Respiratory Distress Syndrome
CITATION: Fridrich P, Krafft P, Hochleuthner H, and Mauritz W.
The effects of long-term prone positioning in patients with trauma-induced adult
respiratory distress syndrome. Anesth Analg, 1996 Dec;83(6): 1206-1211.
During the period from July 1, 1992, to December 31, 1994, all patients with trauma
-induced ARDS [on VENTILATORS] were prospectively studied if they met our study
entry criteria … Earlier turning back to the supine position [from the prone position]
was permitted in emergencies (e.g., loss of airway or venous access, cardiopulmonary
resuscitation) or if the patient did not tolerate the position change. … In all patients,
air cushion beds (Thera-PulseTM bed, KCl-Mediscus, Inc., San Antonio, TX)
were used throughout the study.
This article was originally posted February 10, 2006.
When Is A Patient Prone For Prone? [Editorial Letter]
CITATION: Pappert D, Falke KJ. When is a patient prone for prone?
[Editorial Letter] Anesth Analg 1996 Dec;83(6):1139-40.
This article was originally posted February 10, 2006.
in Obese Patients During General Anesthesia
CITATION: Pelosi P, Croci M, Calappi E, Mulazzi D, Cerisara M, Vercesi P, Vicardi P, Gattinoni L.
Prone positioning improves pulmonary function in obese patients during general
anesthesia. Anesth Analg 1996 Sep;83(3):578-83.
[CHAS’ underlines] In obese patients, anesthesia and paralysis negatively affect
respiratory mechanics and oxygenation more than in normal subjects (2); thus, it has been
hypothesized that the prone position should be avoided whenever possible (3) and/or
exercised with extreme care (4). … We demonstrated that the prone position, if
correctly performed assuring free abdominal movement, is safe in [anesthetized and
paralyzed] obese patients, since it [“increases lung volume, lung compliance, and
oxygenation” and]improves pulmonary function.
This article was originally posted February 10, 2006.
Cardiovascular Parameters in Healthy Volunteers
CITATION: Wadsworth R, Anderton JM, Vohra A. The effect of four different surgical
prone positions on cardiovascular parameters in healthy volunteers.
Anaesthesia. 1996 Sep;51(9):819-22.
Sorry! I couldn’t find a copy of this article when first searching for it. And, knowing what
I know now, even if I someday find it I probably won’t buy it. Here is its entire ABSTRACT:
Twenty healthy volunteers were placed in four different surgical prone positions: on
pillows, on an evacuatable mattress, on pelvic props and in the knee-chest position. The
normal supine position was used as a control for the measurement of cardiovascular
parameters. Mean arterial pressure was measured by automated oscillotonometry.
Transthoracic electrical bioimpedance was used to measure cardiac output and heart rate.
Cardiac index and total vascular resistance index were derived from these data. No
significant changes in heart rate or mean arterial pressure occurred when the volunteers
were moved from the supine position to any of the four prone positions or when returned
to the supine position again. Cardiac index decreased significantly on going from the
supine to the knee-chest position (20%) and onto the props (17%) but not onto the
evacuatable mattress (11%) or the pillows (3%).
This abstract was originally posted February 10, 2006.
Respiratory Mechanics While Improving functional Residual Capacity
and Increasing Oxygen Tension
CITATION: Pelosi P, Croci M, Calappi E, Cerisara M, Mulazzi D, Vicardi P, Gattinoni L.
The prone positioning during general anesthesia minimally affects respiratory mechanics
while improving functional residual capacity and increasing oxygen tension.
Anesth Analg. 1995 May;80(5):955-60.
[CHAS’ underlines] We investigated the effects of the prone position on the mechanical
properties (compliance and resistance) of the total respiratory system, the lung, and the
chest wall, and the functional residual capacity (FRC) and gas exchange in 17 normal,
anesthetized, and paralyzed [intubated and ventilated] patients undergoing elective
surgery. … the patients were positioned prone, assuring free abdominal movements with
upper chest and pelvic supports as suggested by Smith (12).
“Smith (12)” is posted below: Smith RH. One solution to the problem of the prone
position for surgical procedures. Anesth Analg. 1974;53:211-24.
This article was originally posted February 10, 2006.
A LETTER to the EDITOR Re: Pelosi et al’s May, 1995 Anesth Analg study article:
Prone Position and Oxygenation
CITATION: Nishikawa T. Prone position and oxygenation. Anesth Analg. 1996 Apr;82(4):885.
This article was originally posted February 10, 2006.
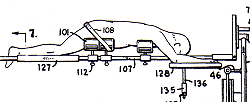
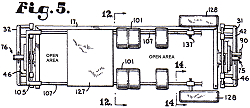
CITATION: Smith RH. One solution to the problem of the prone position for surgical
procedures. Anesth Analg. 1974 Mar-Apr;53(2):221-4.
[CHAS’ underlines] It may be necessary to support 300 or more pounds as much as
12 inches off the operating table simply to free the abdomen for adequate
ventilation. … the kidney rest is elevated, by cranking, as much as is necessary to
raise the abdominal wall off the table, and a pile of folded sheets as high as the pelvis
elevation is placed under the chest … This pattern of support frees the abdomen
completely of all pressure against the table …
Here are the titles and the DATES of Smith’s 2 references cited at the end of his report:
“Problems related to the prone position for surgical operation;” 1961!
“Hoist for the Georgia prone position;” 1964!
Sorry for the pdf file of krappy photocopies. I had to order this article via
“LOANSOME DOC.” So, I could only scan what I was sent.
This article was originally posted February 10, 2006.
To Return To Wherever You Came From
OR Use the Following Links: Email Charly at: chas@novelholiday.com
web counter