
 |
 |
of Frequently Misinterpreted and Misrepresented Restraint Research PART ONE |
CITATION:
Miller CD. A comprehensive review of frequently misinterpreted and
misrepresented restraint research; Part one. February, 2005.
http://www.charlydmiller.com/LIB05/2005chasresearchreviewpart1.html
 NEW as of December, 2005:
NEW as of December, 2005:
A 39-page PDF FILE containing All 3 Parts & the References!
If you're going to PRINT any part of this 3-part Comprehensive Review, print from the PDF file. The webpages end up printing weird (text next to photos bumps the photos to another page). Plus, printing all these parts and the reference list from the webpages takes up a lot more than 39 pages.

ARTICLE #1:
Chan TC, Vilke GM, Neuman T, Clausen JL.
RESTRAINT POSITION AND POSITIONAL ASPHYXIA
Ann Emerg Med, November 1997;30:578-586.(1)
The "Restraint Position and Positional Asphyxia" (RPPA) clinical study that generated this article was developed and conducted some time in 1996 by Dr.s Theodore C. Chan, Gary M. Vilke, Tom Neuman, and Jack L. Clausen. Dr.s Chan, Vilke, and Neuman were of the Emergency Medicine Department, University of California San Diego Medical Center (UCSD), San Diego, California. Dr. Clausen was of the UCSD Pulmonary Medicine Department.(1)
RELATED BACKGROUND INFORMATION
The UCSD RPPA study was initiated by Neuman at the personal request of San Diego County Deputy Counsel, Ricky R. Sanchez, specifically for the purpose of developing evidence to assist Sanchez in defending two San Diego County Sheriff Deputies against a "wrongful-death lawsuit" filed by the survivors of Daniel Price, a man who died while being hogtied and kept in a forceful-prone-restraint position by them in 1994.(2) In fact, Sanchez arranged for San Diego County to pay for the study.
Evidence Now Shows" Obviously, one cannot trust "facts" presented in a newspaper article. Since then, however, I've obtained LEGAL DOCUMENTS wherein both Dr.s Neuman and Chan corroborate the study-generation information reported in the 1998 San Diego Union-Tribune article.(3-6)Furthermore, the official Price v San Diego report also corroborates the 1998 San Diego Union-Tribune article study-generation information.(2) |
|
 |
Neuman has also testified that – in spite of his lack of knowledge regarding this subject – he was asked by Sanchez to be an "expert" witness specifically for the purpose of discrediting decades of restraint-related research published by reputable forensic pathologists (Reay et al), in order to assist Sanchez's defense of two San Diego County Sheriff Deputies.(3)After evaluating some restraint asphyxia materials provided him by Sanchez, Neuman advised Sanchez that a new study would need to be performed in order for Neuman to discredit Reay et al's materials, and that Sanchez would have to provide the funds to accomplish such a study.(3) Sanchez agreed to do so, and soon thereafter the County of San Diego provided UCSD with $33,900.00 to fund Neuman's study.(6,7) [In deposition, Chan refers to this funding as a "GRANT" from the County of San Diego.(8)]Chan has testified that, because Neuman (a UCSD "senior faculty" member) was too busy to do so, Neuman asked him to develop, organize, and direct the study.(8) That is why Chan's name appears first in the study report's list of authors.In deposition, Chan described being personally introduced to Sanchez at a restaurant luncheon "get-together" hosted by Neuman.(9) Vilke -- another RPPA study co-author -- was among those who attended Neuman's "get-together" luncheon. However, Chan denies remembering any other attendees' names, and denies remembering (for a fact) whether Neuman's "get-together" luncheon occurred before the study was performed – or after the study was performed.(9)Yet, according to Neuman, the average body mass index (BMI) of the "general" population was not researched for the purpose of UCSD study subject selection because, "Mr. Sanchez paid for this study, [so] we were trying to pick a [study] population that looked more towards the type of person that Mr. Price was [the San Diego case victim] as far as size, habitus [BMI], gender."(10) Thus, whether or not Chan was personally introduced to Sanchez prior to the study's design and performance, the fact that only study subjects with a BMI similar to Mr. Price were selected for the UCSD RPPA study indicates that Chan knew of Sanchez's specific needs prior to designing the UCSD RPPA study to accommodate them.BACKGROUND INFORMATION SUMMARY:
BACKGROUND INFORMATION CONCLUSION:
Thankfully, within the peer-reviewed and published report of the UCSD RPPA study, the authors clearly identified the fact that their study's findings cannot be applied to real life situations. Thus, as long as their report is read very carefully, it is unnecessary for readers to have an understanding of its development and performance background information in order to recognize that the study's findings are entirely unhelpful to those concerned about the dangers associated with real life restraint situations.
UNFORTUNATELY, not everyone who reads this study reads it carefully. In fact, many who cite it have never actually read it. Instead, their citation relied entirely upon a misrepresentation of the study's data provided to them by those who claim to be "experts" at interpreting it.
Even more unfortunately, when not faced by their peers (when providing expert reports to attorneys, or when in deposition and trial testimony situations), the authors of this study grossly misrepresent the findings they obtained. [Support for that statement is provided in a later section of this review.]
THE UCSD RPPA STUDY's PUBLISHED INFORMATION(1)
STUDY METHODS
This was a "controlled trial" performed at the University of California San Diego Medical Center's Pulmonary Function Laboratory. The study's 15 subjects were healthy men ages 18 – 40 y/o. Subjects were excluded from the study if they had abnormal lung functions, or if their body mass index (BMI) was greater than 30 kg/m2.
"Two potential subjects were excluded for abnormal screening PFT [Pulmonary Function Test] measurements, and another individual was excluded for BMI greater than 30 kg/m2."
I am 5 feet 9 inches tall, and weigh 200 pounds. My BMI is 30 kg/m2.
To calculate YOUR BMI, go to any of these (or similar) Internet websites:
The National Heart, Lung, and Blood Institute BMI Table
The National Institutes of Health BMI Table
CRESTOR BMI Index Table

"PHASE 1" of the study consisted of performing "Pulmonary Function Tests" (PFT) on each healthy, rested study subject, while he was "randomly" placed in four different positions:
A sitting position.A supine position.A prone position.A "restraint position."
 a "TUNTURI" cycle ergometer |
|
performed on "a cycle ergometer" (a stationary bicycle), each study subject was placed in a sitting position for a 15 minute "rest period." During this first PHASE 2 "rest phase":
|
Next, after another 4-minutes of stationary bicycle exercise, each study subject was placed in a "restraint position"
for a 15 minute "rest period."During this second PHASE 2 "rest phase":
"The results of this study demonstrated significant changes in both
static and dynamic pulmonary function testing with position and exercise."
STUDY METHODS IDENTIFICATION, DISCUSSION & REVIEW
Within the abstract (introduction) of their study, the authors concretely identified their "Study Objective" as being,
"To determine whether the 'hobble' or 'hogtie' restraint positionHowever, within their article's body, the authors admitted that the restraint position they used to conduct their 'hobble' or 'hogtie' restraint study only "closely approximates the restraint position noted in previous studies and case reports in the prehospital setting" – only "closely" approximated the position employed during REAL-LIFE field-application of forceful-prone-restraint with hobble and hogtie restraints.
results in clinically relevant respiratory dysfunction."
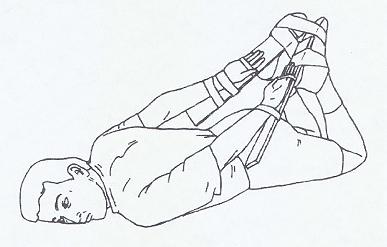
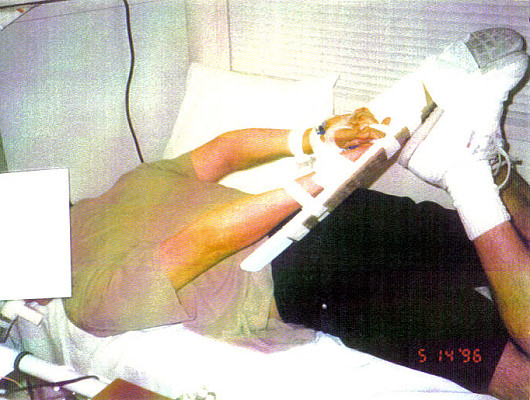
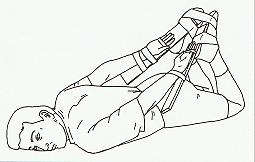
commissioned and published by the authors to demonstrate the "RESTRAINT POSITION" employed for their study. NOT a real-life "hogtie" position. |
|
 |
 |
|
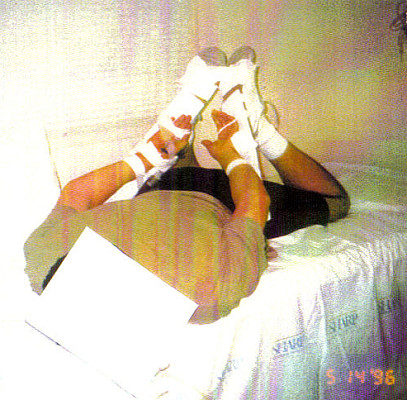
PHOTOGRAPHS of the study position that generated the DIAGRAM Chan et al commissioned for their November 1997 article's Figure 1.
(I have no idea
Again, CLEARLY, |

|
|

|
Note that the SHOULDERS of all individuals shown in "real" hogtie restraint are pulled UP and OFF of the ground. Note that their KNEES are also somewhat pulled UP and OFF of the ground. As you can see; a "real" hogtie position causes someone's ENTIRE BODY WEIGHT to rest upon their ribcage and ABDOMEN. Thus, a "real" hogtie restraint position interferes with the ability of the DIAPHRAGM (the largest muscle of respiration) to easily contract and descend into the abdomen, because it interferes with the room available for the abdominal contents to get out of the way of the descending diaphragm. Consequently, a "real" hogtie restraint position seriously increases the amount of effort required in order for hogtied individuals to breathe – even without "force" being actively applied to their torsos while they are kept in a prone position.
The differences between the "real" hogtie position and the UCSD RPPA's "restraint position" were ignored (apparently considered inconsequential) by the study authors, but these differences are physiologically significant.
The UCSD RPPA study "restraint position" clearly allowed the healthy study subjects' shoulders and knees to comfortably reach and rest upon the floor. Thus, the subjects' shoulders and knees had the ability to assist in supporting (distributing) their body weight, diminishing the amount of weight that had to be supported by the subject's ribcage and abdomen.
Since no force was being applied to his prone body, if any UCSD RPPA study subject experienced any difficulty breathing while in the study's restraint position, he easily could have slightly flexed his shoulders or his knees (or both), compressing them against the ground so as to elevate his ABDOMEN and allow more room for his abdominal contents to move out of the way of his descending diaphragm. Thus, unlike truly hogtied individuals, each study subject had the ability to afford his diaphragm better room to contract and descend into the abdomen – allowing him to breathe better and with much less effort. Additionally, Chan admits that it is unlikely that he or the other study researchers would have noticed (or REPORTED) such a minor – but significant – amount of shoulder- and/or knee-flexion.(11)
To justify their study's failure to use a real hogtie restraint position, Chan et al cited their need "to allow secure placement of a radial artery [IV] line." It is true that the radial artery (the wrist artery) is the safest artery to use in order to obtain arterial blood gas samples. However, in a controlled environment such as the University of California San Diego Medical Center's Pulmonary Function Laboratory, the BRACHIAL artery (the one on the "inside" of the elbow) could also have securely and safely been used. In fact, because the brachial artery is easy to access even when someone is placed in a real hogtie restraint (especially when the person is cooperative with restraint – such as the UCSD RPPA study subjects were), using the brachial artery would easily have allowed Chan et al to use a true form of hogtie restraint for their study.
But, because the UCSD RPPA study authors ELECTED to use an artery that allegedly interfered with them being able to study a real hogtie restraint position, the study's findings clearly are NOT RELATED to the authors' purported "STUDY OBJECTIVE": that of determining "whether the 'HOBBLE' or 'HOGTIE' restraint position results in clinically relevant respiratory dysfunction."
Interestingly enough, although they elected to ignore the significant physiological differences between real hogtie restraint and the "restraint position" they used, within their peer-reviewed and published article, the UCSD RPPA study authors identified several OTHER REASONS why their study's findings cannot be applied to real-life situations.
The following are QUOTES from the study's published article:
EXAMINATION OF THE STUDY'S "CONCLUSION":
Even though they neglected to employ a "restraint position" that reproduced the effects suffered by individuals subjected to a true form of hogtie restraint, and in spite of all the other study limitations identified by the authors, "[Chan et al.] measured significant differences in pulmonary function test results between control and restrained individuals."(12)
Yet, in the CONCLUSION of their study's report, the authors wrote:
"By itself, the restraint position was not associated with any clinically relevant changes in respiratory or ventilatory function in our study population of healthy individuals with preserved ventilatory reflexes and normal pulmonary physiology. There is no evidence to suggest that hypoventilatory respiratory failure or asphyxiation occurs as a direct result of body restraint position in healthy, awake, nonintoxicated individuals with normal cardiopulmonary function at baseline."How many ENTIRELY HEALTHY, "awake, nonintoxicated individuals with normal cardiopulmonary function ... and normal pulmonary physiology" have required the application of maximum forms of RESTRAINT (forceful-prone-restraint, with or without hogtying) in real-life ("field") situations?
NONE. That's how many.
 |
|
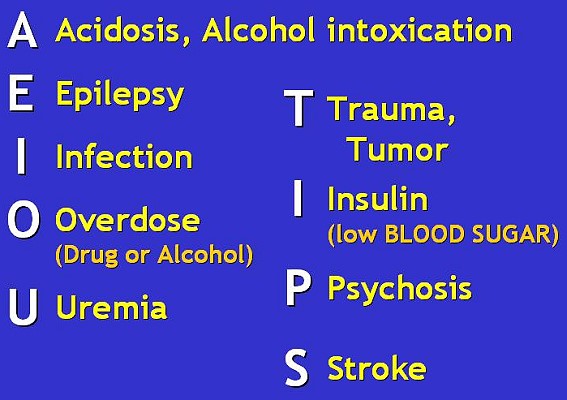
EVER have required application of "maximum" forms of restraint in the field were the victims of SOME sort of
"ALTERED |
MORE "BACKGROUND" INFORMATION:
Excerpts from (Forensic Pathologists) Howard JD and Reay DT.'s
Excerpts from a statement sent to me by Dr. Reay in June, 1998(13);
Excerpts from Dr.s Vilke, Chan, and Neuman's
Excerpts from Vilke et al's Letter:
MORE "BACKGROUND" INFORMATION:
When writing an article for submission to a professional journal, researchers must pen their statements very carefully, because they know their article will be "peer-reviewed" prior to being accepted (or rejected) for publication. In fact, according to Chan, the Annals of Emergency Medicine peer-reviewers provided UCSD RPPA study article authors with critical suggestions causing them to rewrite sections of their article (better identifying the limitations of their study's results), so as to win the approval of the peer-reviewers and gain their study's Annals of Emergency Medicine publication.(15)
All of the following excerpts are from legal documents associated with cases involving deaths due to restraint asphyxia. In each of these cases, the UCSD RPPA study authors who are quoted had been hired by the attorney(s) charged with defending persons who had restrained an individual in a manner that led to his death.
UNITED STATES DISTRICT COURT, San Diego, California:
Quotes from the Final Report of PRICE v SAN DIEGO:
Quotes from the Final Report Attributed To NEUMAN's Trial Testimony Provision:
Romero vs. Rural Metro et al. Cause No. 335185
Moore vs. Guardian Protective Services, INC, and Rural Metro of North Texas, L.P.
Kapanak vs. City of Phoenix; Superior Court of the State of Arizona;
Same Deposition Transcript as above: page 88, lines 6-13:
Same Deposition Transcript as above: page 89; lines 14-25:
Same Deposition Transcript as above: page 101; lines 16-24:
Same Deposition Transcript as above: pages 182-183; lines 19-25, 1-8:
The Only TRUE CONCLUSIONS that can LEGITIMATELY be
Based upon a review of this study's methods, its content, its pre- and post-publication background information, and the post-publication testimonies provided by the study's authors;
NOW, Go To:
A Comprehensive Review of Frequently Misinterpreted and
A Comprehensive Review of Frequently Misinterpreted and
REFERENCES for ALL PARTS of:
RELATED LETTERS PUBLISHED AFTER the STUDY's PUBLICATION
Letter to the editor re. Restraint position and positional asphyxia
Annals Of Emergency Medicine July 1998; 32(1):116-117.(12):
[Chan et al.] measured significant differences in pulmonary function test results between control and restrained individuals, but describe the changes as "not clinically relevant." ...
Restrictive pulmonary function alteration that may not be "clinically relevant" might well be one of several contributing factors in some deaths where restraint is used. ...
Applying only "clinically relevant" values to a measurement may lead to misinterpretation of findings in deaths that occur outside the clinical setting.
Reay DT. Hog-Tied Revisited
http://www.charlydmiller.com/LIB/reaysdiego.html:
[Chan et al's] study showed that our study in 1988 (Am J Forensic Med Pathol 1988;9:16-18), which measured only cutaneous (skin) oxygen saturation, was incorrect and flawed and our interpretation that hog tying produces physiological consequences of recovery times as measured by pulse and oxygen saturation was contradicted by their work.
I readily acknowledged the value of [Chan et al's study] ... This has since been presented in law enforcement publications as my retraction of positional asphyxia as a cause of death, with particular reference to hog-tying.
Such is not the case! I still maintain that there are risks and hazards to restraint maneuvers including hog-tying and each case must be evaluated to assess the presence or absence of respiratory restriction in the light of the method of restraint.
A 280-pound man with a large [belly] is at risk in the face down position as well as a person with obstructive pulmonary disease. And there are many shades in between.
The point is that street deaths are much different than controlled investigations. If 14% respiratory restriction by hog-tying is not viewed as clinically significant in normal people, it has to be evaluated in the context of the event where it may be significant.
Letter to the Editor Re: Patient restraint in EMS
and the "Patient restraint in EMS" AUTHORS' REPLY;
Prehosp Emerg Care July/September 2003;7(3):417-419.(14)Kupas and Wydro state that "patients should never be transported while hobbled, 'hog-tied,' or restrained in a prone position (which) has been associated with asphyxia." ... Reay has retracted his conclusions about the physiologic effects of the hobble position based on "more comprehensive" clinical research. [Vilke et al cite their UCSD RPPA study here.] This new research included a study by Chan et al. in which subjects were placed in the sitting, supine, prone, and hobbled positions with spirometric, arterial blood gas, pulse oximetry, and cardiovascular monitoring, in which no significant change to suggest increased risk for asphyxiation was demonstrated."
Excerpts from Kupas and Wydro's Reply to Vilke et al.:
Vilke and colleagues express a concern that there is not firm evidence associating deaths in restrained individuals to the prone or hobble positions. ... Despite their comments, Vilke et al. do not make any statement that advocates for the general use of these positions during restraint of violent patients.
... [Note that] none of the physiologic studies related to the prone or hobble positions [cited by Vilke et al] were performed on individuals who were violently struggling against the restraints or were under the influence of adrenergic or sedating drugs. We do not know what effect other medical conditions, psychiatric conditions, violent agitation, or drug intoxication would have on the physiologic effects of prone or hobble restraint positions.
Vilke and colleagues also suggest that "Given the numbers of cases of sudden death that occur to restrained individuals in all positions, we would recommend rhythm monitoring, when possible, in all restrained patients with frequent cardiopulmonary assessments as well." This statement is further reason to avoid prone or hobble restraint positions, because cardiopulmonary assessments are more easily accomplished when the patient is in the supine position.
We still believe that patients should never be transported while hobbled, "hog-tied," or restrained in a prone position with hands and feet behind the back.
TESTIMONIES PROVIDED by STUDY AUTHORS AFTER
THE UCSD RPPA STUDY WAS PUBLISHED
However, when NOT faced by their "peers" – when providing expert reports to attorneys, or when providing deposition or trial testimony – UCSD RPPA authors have grossly misrepresented their study's findings.
As you read these excerpts, keep in mind that; within the peer-reviewed 1997 publication of their 1996 UCSD RPPA study's report, Chan et al freely admitted that their study's findings CANNOT be applied to real life situations.
Ann PRICE et al., v. County of San Diego et al. January 8, 1998.
"FINDINGS OF FACT AND CONCLUSIONS OF LAW"(2):
On June 30, 1994 Price died. A county medical examiner, John W. Eisele, M.D., conducted the autopsy. Dr. Eisele found low levels of methamphetamine in Price's system. He also found petichaie (pinpoint) hemorrhaging in Price's left eye, which suggests that Price's torso had been compressed. Dr. Eisele listed the cause of death as "hypoxic encephalopathy due to restrictive asphyxia with cardiopulmonary arrest due to maximum restraint in a prone position by law enforcement."
Dr. Eisele testified that Price experienced lactic acidosis. ... Dr. Eisele testified that because the hogtie restraint impairs the mechanical process of exhaling, it prevents the body from "blowing off" excess carbon dioxide. In other words, Dr. Eisele opined that Price suffered from asphyxia (an increase in carbon dioxide levels) that, because of the hogtie, Price's body could not correct.
After Price's death, at the request of defense counsel, Thomas Neuman, M.D., of the University of California at San Diego Medical Center ("UCSD") conducted a sophisticated study of positional asphyxia and the hogtie restraint. Dr. Neuman found ... that although the hogtie restraint impairs the mechanical process of inhaling and exhaling to an extent, the hogtie does not affect blood oxygen or carbon dioxide levels. In other words, the impairment is so minor that it does not lead to asphyxia, and in fact has no practical significance.
The UCSD study also refutes Dr. Eisele's opinion that the hogtie prevents the lungs from "blowing off" excess carbon dioxide.
As Dr. Neuman testified, it is wild speculation to say that a person lying prone with a potbelly will asphyxiate to death ...
Dr. Neuman perfectly captured the cause of death when he made the following statement: We have clear data that there is no respiratory component to the hogtie position.
in the Superior Court of the State of Arizona, in and for the County of Pima.
Quotes from a sworn affidavit written by Dr. Theodore Chan (in lieu of submitting an "Expert Report"),
and signed under oath on April 27, 2001:
4. I was directly involved in the research study performed at UCSD, funded by a grant from the County of San Diego for the specific purpose of examining the issue of positional restraint as it relates to pulmonary function and specifically the effect of the hobble restraint on respiratory function.
...
7. In the matter of Romero v City of Tucson; Rural Metro, et al., I was requested ... for my opinion concerning the impact of hobble or partial hobbled restraint of Mr. Romero and what role, if any, it played as a cause of his death.
...
8. It is my opinion, within a reasonable degree of medical probability [based upon the UCSD RPPA study], that the position in which Mr. Romero was restrained and then transported to the Emergency Department of Kino Hospital did not compromise Mr. Romero's respiration and, therefore, played no role in causing death from respiratory failure, arrest or asphyxiation.
(MEDSTAR Ambulance); Cause No. 17-187577-01;
in the District Court of Tarrant County, Texas, 17th Judicial District;
Transcript of testimony provided by Dr. Tom Neuman,
during a deposition conducted on Sunday, June 23, 2002: page 46; lines 7-19:
...
County of Maricopa; No. CV 2001-012136;
Transcript of testimony provided by Dr. Theodore C. Chan,
during a deposition conducted on Tuesday, August 26, 2003:
page 56; lines 2-8:
...
derived from ARTICLE #1 ["Restraint position and positional asphyxia"(1)]:the following facts are indisputable:
The UCSD RPPA study's "OBJECTIVE" was NOT the one stated by its authors;
"To determine whether the 'hobble' or 'hogtie' restraint position results in clinically relevant respiratory dysfunction."
This study's TRUE OBJECTIVE was
"To afford Dr. Tom Neuman the means to provide testimony that could be INFERRED as discrediting decades of restraint asphyxia research performed by unbiased forensic medical professionals; testimony that could be INFERRED as suggesting that hogtie restraint 'doesn't kill;so as to assist San Diego County Deputy Counsel Ricky Sanchez in his defense of two San Diego County Sheriff Deputies accused of causing the "wrongful-death" of a man who died while being hogtied and kept in a forceful-prone-restraint position by them in 1994."
Misrepresented Restraint Research; PART TWO
Chan TC, Vilke GM, Neuman T.
Reexamination of custody restraint position and positional asphyxia
Am J Forensic Med Pathol, September 1998;19(3):201-205.
Posted in March, 2005.
Misrepresented Restraint Research; PART THREE
Chan TC; Neuman T; Clausen J; Eisele J; Vilke GM.
Weight force during prone restraint and respiratory function
Am J Forensic Med Pathol, September 2004;25(3):185-189.
Finally posted on August 1st, 2005!
A Comprehensive Review of Frequently Misinterpreted and
Misrepresented Restraint Research
SECOND DRAFT Posted in March, 2005.
To Return To Wherever You Came From
OR Use the Following Links:
Misrepresented Restraint Research Article MAIN PAGE Email Charly at: c-d-miller@neb.rr.com
Email Charly at: c-d-miller@neb.rr.com
(Those are hyphens/dashes between the "c" and "d" and "miller")

