
 |
 |
by Traumatic Asphyxia |
|
 |
CITATION:
Miyaishi S, Yoshitome K, Yamamoto Y, et al.
Negligent homicide by traumatic asphyxia.
Int J Legal Med Jan 14 2004.
The International Journal of Legal Medicine
is the Official Publication of the International Academy of Legal Medicine.
CHAS' "REVIEW": My comments are FEW.
So, rather than write a separate "review," my comments are inserted in blue print where relevant.
Case Report
Negligent Homicide by Traumatic Asphyxia
S. Miyaishi, K. Yoshitome, Y. Yamamoto, T. Naka, and H. Ishizu
The authors all are from the Department of Legal Medicine,
Okayama University Graduate School of Medicine and Dentistry,
2-5-1 Shikata-cho, 700-8558; Okayama, Japan.
Received: 12 May 2003; Accepted: 1 December 2003; Published Online: 14 January 2004.
Abstract We presented an unusual case of negligent homicide by thorax compression, which is the expanded concept of traumatic asphyxia. A 58-year-old man was restrained in the prone position by six prison officers. They were ordered by their superiors to continue restraining him for about 15 min and the victim died. At the forensic autopsy, typical findings of thorax compression with intramuscular hemorrhages on the back and multiple fractures of the ribs were observed. No evidence of neck compression/smothering or other fatal issues likely to occur by chest compression was found. The reconstruction of the scene corresponded exactly with the localization of the injuries found in the victim. This is the first case of death by pure thorax compression without other fatal factors during intentional restraint, in which the force causing the chest compression was distinctly determined by the autopsy and reconstruction.
Keywords Thorax compression - Traumatic asphyxia - Negligent homicide.
[Keywords should also include "restraint asphyxia."]

Introduction
It is well known that thorax compression occurs in cases where an individual is buried alive by disaster, is pinned to a wall by a car while repairing it, or other similar situations [1, 2, 3, 4, 5, 6]. Accidental death from chest compression may also occur when an adult rolls onto an infant while sleeping or when someone falls down in a narrow space. A very rare case of asphyxia by thorax compression was also reported where an infant died when a python tightened around it [1].
In the pathophysiology of traumatic asphyxia according to Perthes [7], reflexive closure of the epiglottis with simultaneous tension of the abdominal muscle has been found to be a very important mechanism for increasing the intrathoracic pressure along with the subsequent findings. However, traumatic asphyxia is now generally defined as a type of asphyxia caused by chest (or upper abdomen) compression, which does not include the pathogenesis described. For example, Knight stated that "it (traumatic asphyxia) is well recognized now as meaning mechanical fixation of the chest" [4]. Di Maio described "traumatic asphyxia occurs when a large weight falls onto or presses down on an individual's chest or upper abdomen, making respiration impossible" in his textbook for forensic pathology [1]. In this paper, we present an unusual case of negligent homicide (according to the Japanese law) by traumatic asphyxia, which occurred during the restraint of a victim by six prison officers.
["Traumatic asphyxia" caused by RESTRAINT IS "restraint asphyxia."]
Case history
A 58-year-old man who had visited an inmate in prison got into trouble with the prison officers. The prison warden ordered him to leave the prison, but the visitor disobeyed this order and assaulted the warden. Although the man was immediately arrested for obstructing the warden in the performance of his duties, he reacted extremely violently. Therefore, six prison officers immediately restrained him in the prone position. According to the statements of the prison officers, the victim lost some of his strength in 1-2 min after being restrained and nearly completely in 7-8 min. After about 10 min passed, the victim showed no signs of resistance, yet the prison officers had to keep restraining him following the order of their superiors, who had inspected the situation. After 14-15 min had passed, a policeman arrived at the scene and the prison officers relaxed their restraint on the victim. The victim had already undergone cardiopulmonary arrest.
Autopsy findings
The victim was somewhat obese (160 cm in height and 64 kg in weight) and had a potbelly. The face, neck and upper part of the chest were congested and many petechiae were observed on the conjunctivae and skin around the eyelids (Figs. 1 and 2). Neither abrasions around the nose or mouth nor any traces of external force on the neck were noticed. Intramuscular bleeding without subcutaneous hemorrhage was observed in the upper part of the right scapular region and the outside of the left infrascapular region (Fig. 3). Some small subcutaneous hemorrhages were also observed in the extremities. Cardiac blood was cyanotic and highly fluid, many subserosal petechiae were seen in both lungs and all organs were severely congested. The right first through fourth ribs were fractured adjacent to the spine, the first and ninth ribs on the left side were also broken. These fractures were accompanied with bleeding in the surrounding soft tissues (Fig. 4). Although some pathological changes such as arteriosclerosis and liver cirrhosis were observed, they were so slight that they could not contribute to the fatal outcome.

Fig. 1 General appearance of the victim |
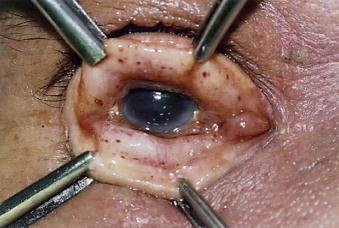
Fig. 2 Petechiae observed in the |

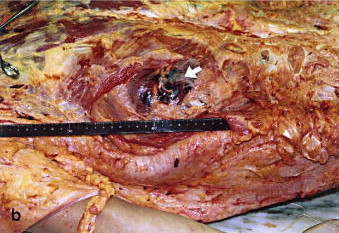
Fig. 3 Intramuscular bleeding in the back of the victim,
(a) right scapular region, (b) left infrascapular region.
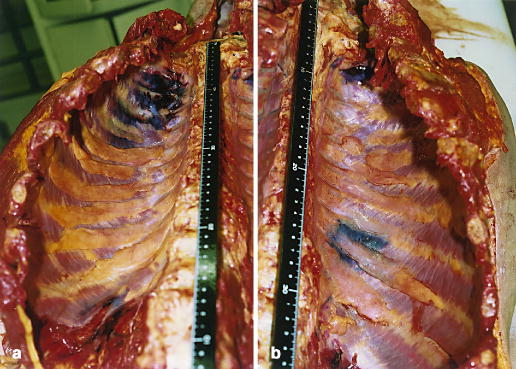 |
accompanying the bleeding in the surrounding soft tissues; (a): right first through fourth ribs and (b): left first and ninth ribs. |
The histological examination revealed some typical findings of asphyxia, for example, interstitial and hemorrhagic alveolar edema of the lungs, polynuclear giant cells in the alveolar lumen, vacuolization of hepatocytes. Fat and bone marrow embolisms as described by Brinkmann were also observed [8].
Reconstruction of the scene
The situation of the restraint was reconstructed in the criminal investigation. Six prison officers (Fig. 5; A-F) ganged up immediately and simultaneously to restrain the victim after he had acted violently against the arrest. The victim was in the prone position with his right arm under his chest and three officers restrained the back and the other three restrained only the extremities. The situation reconstructed separately for each officer was as follows (Fig. 5): Officer A held the left arm of the victim under the right arm and put the weight on the left side of the victim's back (Fig. 5a), Officer B pressed the right shoulder of the victim using the right knee (Fig. 5b), Officer C restrained the victim by holding the center of the victim's back and the waist from the right side (Fig. 5c), Officer D held the waist and the right ankle of the victim at first, and then the site of restraint was changed from the waist to the right popliteal region (Fig. 5d), Officer E bent the left knee of the victim and put the weight on the shank (Fig. 5e), Officer F held the victim's left wrist to help Officer A at first (Fig. 5f), and then he moved to restrain the left ankle of the victim. No one held the neck region of the victim and there was nothing around his nose or mouth to prevent respiration.

Discussion
The following are examples of cases where traumatic asphyxia is known to occur: landslide or avalanche, collapse of stones in mines, haystack falling in a silo or sand from a hopper, falling timber or masonry, and crushing by other bodies in a panicked crowd. In these typical cases of traumatic asphyxia there are two characteristics. The first is that the force acting on the victim is significant. The other is that death is caused by an unexpected disaster. From these viewpoints, our case is obviously different than the typical traumatic asphyxia.
In the present case, six prison officers restrained the victim, but only three of them pressed the chest of the victim.* Although Knight referred to a scenario similar to the thorax compression in our case [4], he introduced only one practical case in the former edition of his book, in which six large officers had piled on top of the victim [9]. The force acting on the victim in our case was believed to be much smaller as compared with the typical cases of traumatic asphyxia. Based on the relatively small force used in this case for chest compression*, reflexive closure of the epiglottis and tension of the abdominal muscle might occur uncertainly. The autopsy findings indicating traumatic asphyxia in the present case were not so remarkable: for example there were no petechial bleeding of the whole face, neck and shoulders. Since relatively slight chest compression was used, the superiors of the six prison officers who were in charge of the order to restrain the victim, may have judged the risk of traumatic asphyxia incorrectly. A further misjudgment of the situation may have derived from the fact that the nose and the mouth of the victim were not blocked. Many people believe that asphyxiation could not occur in this type of situation. It could be denied that the superiors had not noticed the sudden death which may occur following localized short term blunt force to the chest as pointed out by Darok et al. [10] because he had furiously resisted for some minutes from the beginning of the restraint.
[ * "Chest" compression is a minimal contributor to restraint asphyxia. It is ABDOMINAL compression (especially during forceful-prone-restraint) that is the most significant cause of restraint-related respiratory failure and subsequent asphyxia.]
The second characteristic of the present case was that the victim died solely from traumatic asphyxia caused not by disaster but by intentional restraint. It has been pointed out that traumatic asphyxia may occur as a homicide by kneeling or sitting on a victim, but no practical cases have been reported.** In one similar fatal case described by Knight [9], the restraint of the victim had occurred after the event and the purpose had not been to restrain but to apply handcuffs. In the case reported here, the purpose of restraining the victim was the restraint itself.
Many cases of accidental death during restraint in the prone position have been reported [11, 12, 13, 14]. In these cases, however, other factors or mechanisms of death played important roles as well as the compression of the chest. These factors included compression of the neck, intoxication with illicit drugs, alcohol or psychotropic agents, psychiatric or drug-induced state of agitated delirium, or internal diseases. In only one case was traumatic asphyxia thought to be the cause of death. However, the victim had been in a state of mental disorder and the description did not refer to the effect of psychotropic agents, delirium or other factors.**
[ ** The definition of "restraint asphyxia" does not require neck compression, alcohol or drug intoxication, states of agitated delirium, internal diseases, or the like. Clearly, these kinds of factors will increase the likelihood of restraint asphyxia occurring. (Obesity, or a "pot belly" also increases restraint asphyxia risk.) But, restraint asphyxia is NOT dependent upon such factors. All "restraint asphyxia" requires is that an individual dies as a result of being in a position that prevents adequate breathing, that RESTRAINT was the reason for the individual's inability to escape the asphyxiating position, and that there are no other medical or traumatic findings that could have (by themselves) caused death. Thus, this case study IS a "restraint asphyxia" case study.]
Keeping a person in a prolonged hogtied position or forcing the arm backward were also discussed as factors that restrict the respiratory movement. Some authors proposed that for these cases, the concept of "restraint asphyxia" or "positional (postural) asphyxia" be applied to discriminate them from traumatic asphyxia [4, 12, 13]. The cause of death in the present case, however, was determined to be traumatic asphyxia without other fatal factors. The general findings of asphyxia and injuries traced to the external force were clearly revealed at the autopsy. No evidence of neck compression, use of drugs, alcohol, or other causes that could lead to death were found.
[See ** note above this paragraph.]
Often no injury is observed during the autopsy after traumatic asphyxia. In the present case, however, intramuscular hemorrhages and rib fractures were found as evidence of restraint and their localization was consistent with the reconstruction of the scene. Intramuscular hemorrhage in the left infrascapular region and fractures of the left first and ninth ribs could have been made by the restraint of Officer A, and hemorrhage in the right scapular region and fractures of the right first through fourth ribs could be identified as the injuries caused by the kneeling of Officer B. The localization of subcutaneous hemorrhages in the extremities of the victim was also in accordance with the reconstructed situation. To our knowledge, this case is the first report of traumatic asphyxia where the trace of the force causing the chest compression could be obviously demonstrated by the autopsy in combination with the reconstruction.
In the present case, the legal responsibility of the prison officers and their superiors was evaluated. The six prison officers who restrained the victim felt that he might die, but they had to continue restraining him, because they were ordered to do so. In prisons, superiors have absolute authority over their subordinates, and subordinates who disobey orders are punished. The superiors who gave the order to restrain the victim were not aware that the victim was dying, although they made rounds to inspect the situation. Yet they were ignorant about the danger of restraining a person. The prosecution dropped charges against the six prison officers in consideration of these circumstances and according to Japanese law. However, the three superiors, including the warden of the prison, were indicted for professional negligence resulting in death. As a result of the trial, fines were imposed on all three superiors on the above charge (professional negligence resulting in death).
References
(1) Di Maio DJ, Di Maio VJM (1993) Forensic pathology. CRC Press, Boca Raton.
Pages from the ASPHYXIA chapter of DiMaio & DiMaio's Forensic Pathology, 2nd ed. (© 2001) are in Charly D. Miller's Restraint Asphyxia Library. Traumatic asphyxia is addressed there.
(2) Gresham GA (1993) Violent forms of asphyxial death. In: Mason JK (ed) The pathology of trauma. 2nd ed. Edward Arnold, London, pp 204-213.
(3) Spitz WU (1993) Compression of the chest. In: Spitz WU (ed) Spitz and Fishers medicolegal investigation of death, 3rd ed. Charles C Thomas, Springfield, pp 484-485.
(4) Knight B (1996) Forensic pathology. 2nd ed. Arnold, London.
(5) Hambeck W, Püschel K: Death by railway accident: incidence of traumatic asphyxia. J Trauma 1981, 21:28-31.
(6) Grellner W, Madea B: Zum Tod durch Perthessche Druckstauung. Arch Kriminol 1996, 198:167-175.
(7) Perthes C: Ueber ausgedehnte Blutextravasate am Kopf infolge von Compression des Thorax. Dtsch Z Chir, 1899, 50:436-443.
(8) Brinkmann B: Zur Pathophysiologie und Pathomorphologie bei Tod durch Druckstauung. Z Rechtsmed, 1978, 81:79-96.
(9) Knight B (1991) Forensic pathology, 1st ed. Edward Arnold, London.
(10) Darok M, Beham-Schmid C, Gatternig R, Roll P: Sudden death from myocardial contusion following an isolated blunt force trauma to the chest. Int J Legal Med 2001, 115:85-89.
(11) OHalloran RL, Lewman LV: Restraint Asphyxiation In Excited Delirium. Am J Forensic Med Pathol, 1993, 4:289-295.
(12) Chan TC, Vilke GM, Neuman T: Reexamination of Custody Restraint Position and Positional Asphyxia. Am J Forensic Med Pathol, 1998, 19:201-205.
(13) OHalloran RL, Frank JG: Asphyxial Death During Prone Restraint Revisited: a report of 21 cases. Am J Forensic Med Pathol, 2000, 21:39-52.
(14) Siebert CF, Thogmartin JR: Restraint-Related Fatalities in Mental Health Facilities: report of two cases. Am J Forensic Med Pathol, 2000, 21:210-212
 Email S. Miyaishi at: miyaishi@md.okayama-u.ac.jp
Email S. Miyaishi at: miyaishi@md.okayama-u.ac.jp
CHAS' FINAL COMMENTS:
This is a very interesting case study.
I especially appreciate the restraint position Scene Reconstruction photography. Immediately after getting this posted in my Restraint Asphyxia Library, I will Email the lead author, and ask if – by chance – a photo was taken of ALL SIX of the officers in place, simultaneously. If so, and if I can get it, I'll post it!
The case study didn't mention whether or not resuscitation of the victim was attempted, or whether or not he was transported to an emergency department. If he was transported to an emergency department, I would dearly love to see the lab values obtained from the blood samples obtained there! Did he demonstrate metabolic acidosis? Rhabdomyolysis?
When I Email the lead author, I'll inquire about that also. If there are emergency department lab values available, I'll do my best to get them and post them.

Email Charly at: c-d-miller@neb.rr.com