
 |
in Mental Health Facilities: Report of Two Cases |
CITATION:
Siebert CF, Thogmartin JF. Restraint-related fatalities in mental health facilities: Report
of two cases. Am J Forensic Med Pathol (Sep) 2000, 21(3);210-212.
Siebert, Charles F. Jr. M.D.; Thogmartin, Jon R. M.D.
From the Palm Beach County Medical Examiner's Office, West Palm Beach, Florida, U.S.A.
Manuscript received August 30, 1999; accepted December 10, 1999.
Address correspondence to Charles F. Siebert Jr., 3126 Gun Club Road, West Palm Beach, FL 33406, U.S.A.
ABSTRACT
Mental health facilities are occasionally confronted with patients who display destructive or disruptive behaviors requiring physical restraint. Under these circumstances, restraint can be associated with death. This case report describes two fatalities associated with physical restraint applied by staff members at mental health facilities.
The use of "poseys," restraint chairs, straight jackets, isolation rooms, and medication, among other methods, have been and are being used in mental health facilities as a means of controlling patients with violent and disruptive behaviors. Rarely, restraints result in fatalities.(1) Deaths associated with these restraint devices, as well as manual restraint techniques such as the therapeutic basket hold, carotid sleeper, and various other "holds," have been reported.(2,3)
CASE REPORTS
Case 1
A 29-year-old black man with a long history of schizophrenia and violent episodes, including assaults, was an inpatient at a mental health facility. His only medication was clozapine. He had recently assaulted a female staff member, and his violent outbursts were considered unpredictable.
On the day of the incident, the decedent reportedly began to assault a considerably smaller male staff member. The staff member managed to get behind the patient and hold on to the patient's neck and trunk as pictured in Figure 1. The men ended up prone, with their torsos on a vinyl covered couch. The patient was face down on the couch with his knees on the floor and the staff member holding his neck-shoulder-torso area for 4 to 7 minutes. When other staff members arrived to render aid, the patient reportedly appeared to stand up partially on his own but suddenly went into cardiorespiratory arrest. Cardiopulmonary resuscitation was initiated, and the patient was transported to the local hospital, where life support was terminated 1 week later after he was declared brain dead. The physician who saw the patient on the day of admission described the patient's eyes as "bulging out of his head" and described numerous conjunctival petechiae. The patient was never conscious after the altercation.
 FIG. 1. Diagram of arm hold and body positions in case #1. |
Case 2
A 17-year-old female inpatient at a mental health facility was involved in an altercation with another patient. This was one of several altercations the patient had been involved in during her 2-year history in the facility. The decedent was restrained by two staff members in a "therapeutic basket hold" as pictured in Figure 2. She was tripped and placed prone on the floor with one staff member maintaining the basket hold while lying on top of the patient for what was reported to be between 5 and 15 minutes while the other staff member controlled her feet. She had stopped being combative minutes before, but the hold was maintained because during past episodes of restraint she had "played possum" and continued the altercation after being released. Upon release of the hold, she was found to be unresponsive, and resuscitation efforts were unsuccessful.
 FIG. 2. Diagram of arm hold and body positions in case #2. |
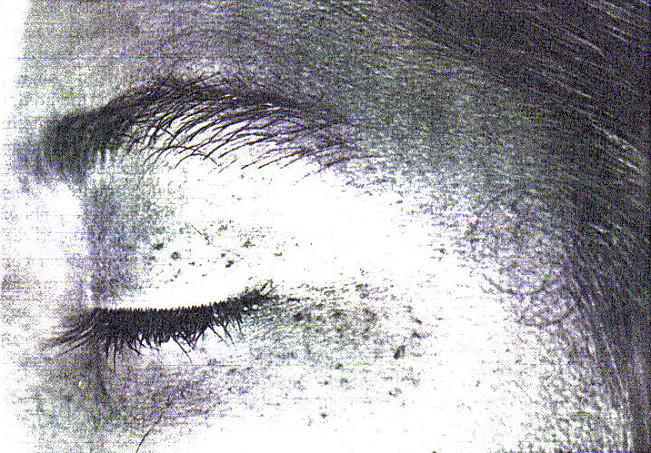
FIG. 3. Prominent periorbital petechiae in case #2.
DISCUSSION
Cases of positional and compressive asphyxia have been well described in the literature. These include deaths of individuals associated with poseys, hogties, bed rails, and choke holds.(2,3) Conjunctival petechial hemorrhages have been described in many cases. Indeed, petechial hemorrhages of the conjunctivae, face, and trunk have been well described in cases of asphyxia involving neck and/or chest compression.(4-6) Being placed in the prone position itself has been associated with sudden death and/or postural asphyxia, particularly in cases associated with excited delirium, drug use, and police custody.(7,8)
A recent media report documented 142 cases of restraint/seclusion-related deaths in mental health facilities in the past 10 years. The report claims that of the 142 deaths, 26% were =17 years of age, whereas this age group constituted <15% of the population housed in mental health facilities. The report claims a statistical estimate of between 50 and 150 such deaths per year.(1)
The 2 cases reported here are similar in that they both involved upper body compression and presented with petechial hemorrhages and a complete lack of natural disease processes that could lead to sudden death. Case #1 involved a violent and possibly life-threatening assault on a staff member at a mental health facility. The hold applied by the staff member was one of last resort and was intended more as a self-defensive act on the part of the staff member than as a therapeutic restraint. The staff member maintained the hold until help arrived. The case is remarkable in that the patient initially recovered from his arrest due to his healthy cardiopulmonary system, only to succumb 1 week later secondary to the severe cerebral hypoxia he was subjected to during the original altercation. The obvious petechial hemorrhages at autopsy in conjunction with the description from the first attending physician and the circumstances surrounding the decedent's final activities leave no doubt that asphyxiation was the underlying cause of the decedent's cerebral anoxia and eventual demise. He had no other medical diagnoses that could account for the petechiae.(9,10) The decedent was exposed to chest compression (the staff member's body weight and arm pressure), airway obstruction (the decedent's face was in the couch), and cerebral blood flow obstruction (the partial neck compression). These three elements proved to be a lethal combination, especially considering the estimated time of application of 4 to 7 minutes.
Case #2 involved a "therapeutic basket hold," which is considered safe if properly applied. The decedent's history of "playing possum" in the past may have lead to the hold being applied for an extended period of time (5-15 minutes), resulting in the asphyxiation of the patient by chest compression. The chest compression involved two elements: the arm wrap across her chest, and the weight of the staff member on top of the patient while she was prone. The decedent had prominent conjunctival and upper body petechiae identical to what has been described in other cases involving chest compression and asphyxia.(11) The petechial hemorrhages ended at the point on the torso where the decedent's arms were wrapped. She also had no cardiac or respiratory findings, history of syncope, or other significant medical conditions.
Both cases reported here involved chest compression holds that were applied for >4 minutes, which could have easily resulted in severe prolonged cerebral hypoxia and death.(12) Grand juries were convened in both cases but failed to indict the individuals involved.

REFERENCES
1. Weiss E, Megan K, Blint DF, Altimari D. Deadly restraint: a Hartford Courant investigative report. The Hartford Courant 1998 CLQ:Oct:11-5.
2. Rubin BS, Dube AH, Mitchell EK. Asphyxial deaths due to physical restraint: a case series. Arch Fam Med 1993;2:405-8.
3. Reay DT, Eisele JW. Death from law enforcement neck holds. Am J Forensic Med Pathol 1982;3:253-8.
4. Spitz WU. Asphyxia. In Spitz WU, ed. Spitz and Fisher's medicolegal investigation of death: guidelines for the application of pathology to crime investigation. Springfield, IL: Charles C Thomas, 1993:444-97.
5. Bell MD, Rao VJ, Wetli CV, Rodriguez RN. Positional asphyxia in adults: a series of 30 cases from the Dade and Broward County Florida Medical Examiner Offices from 1982 to 1990. Am J Forensic Med Pathol 1992;13:101-7.
6. Koiwai EK. Deaths allegedly caused by the use of "choke holds" (shime-waza). J Forensic Sci 1987:32:419-32.
7. Reay DT. Suspect restraint and sudden death. FBI Law Enforcement Bulletin 1996;May:22-5.
8. Steffee CH, Lantz PE, Flannagan LM, Thompson RL, Jason DR. Oleoresin capsicum (pepper) spray and "in custody deaths." Am J Forensic Med Pathol 1995;16:185-92.
9. Jaffe FA. Petechial hemorrhages: a review of pathogenesis. Am J Forensic Med Pathol 1994;15:203-7.
10. Rao VJ, Wetli CV. The forensic significance of conjunctival petechiae. Am J Forensic Med Pathol 1988;9:32-4.
11. DiMaio DJ, DiMaio VJM. Asphyxia. In Forensic pathology. New York: Elsevier, 1989:207-51.
12. De Girolami U, Frosch MP, Anthony DC. The central nervous system. In Cotran RS, Kumar V, Robbins SL, eds. Robbins pathologic basis of disease 5th ed. Philadelphia: WB Saunders, 1994:1295-354.
Keywords:
Forensic science; Restraint; Asphyxia; Petechiae; Death
 Email Charly at: c-d-miller@neb.rr.com
Email Charly at: c-d-miller@neb.rr.com