
 |
 |
and Wedging: A 15-Year Retrospective Study |
THE AMERICAN JOURNAL OF FORENSIC MEDICINE AND PATHOLOGY
2001;22:155-159.
AUTHOR: Kim A. Collins, M.D.
From the Department of Pathology and Laboratory Medicine, Forensic Section, Medical University of South Carolina, Charleston, South Carolina, U.S.A.
CITATION:
Collins KA; Death by overlaying and wedging: a 15-year retrospective study. Am J Forensic Med Pathol (United States), Jun 2001, 22(2) p155-69.

Overlaying, the accidental death by smothering caused by a larger individual sleeping on top of an infant, is a cause of death that has been documented for centuries. The hazard of death has been reported to be greater in infants less than 5 months of age but may occur in children up to the age of 2 years. When an adult or older child rolls on top of an infant, mechanical asphyxia results. The face may be pressed into the mattress or into the body of the sleeping adult or older child. The infant's air may be expressed, and he or she is unable to cry due to pressure on the thorax and the inability to inhale. Some pathologists and investigators believe that the victims of overlaying have no pertinent physical findings at autopsy and that any injury is indicative of inflicted trauma. Others believe that one may see contusions and abrasions from overlaying in and of itself. Wedging is another form of accidental mechanical asphyxia that may have negative autopsy findings. The prevalence of bruising, contusions, or facial and ocular petechiae is not clear.
The author reviewed all pediatric forensic cases referred for autopsy to the Forensic Section of the Medical University of South Carolina/Medical Examiners' Office over the past 15 years, from 1985 to 1999. Of these, all cases of overlaying, cases listed as undetermined sudden infant death syndrome versus overlaying, and wedging were included. The cases were analyzed as to victims' age, sex, race, location/bedding, bed-sharer, and whether the bed-sharer was known to have ingested drugs or alcohol before sleep. Postmortem physical findings were also reviewed, particularly for documentation of contusions, abrasions, or facial or ocular petechiae. By clarifying not only the victim, bed-sharer, and scenario but also the presence or absence of physical findings in cases of overlaying, wedging, and other accidental asphyxia, we can better categorize these cases.
Key Words: Overlaying; Wedging; Infant death
Dangerous sleeping environments have been studied and documented in various reports throughout the world.(1-8) These reports have often led to formal investigations and the formulation of specific safety recommendations. Accidental asphyxia from unsafe surroundings may be secondary to hanging from a curtain cord or clothing, wedging between a mattress and a wall, or airway occlusion from a plastic material.(1,4,6,9,10) During the past decade, many have promoted supine sleeping of infants and the cessation of bed sharing. Studies show that infants sleeping in the same bed as their parents are at an increased risk of death, predominantly by overlaying.(1,7,11-14) A recent study by Nakamura et al. (1) concludes that placing children younger than 2 years of age to sleep in adult beds exposes them to potentially fatal hazards. Despite such research, others question the validity of such conclusions and claim that bed sharing motivates bonding and protection of the infant during sleep.(15) Proponents of bed sharing claim that bed sharing results in increased infant movement during sleep, increased sensitivity of the adult to the presence of the infant, and resultant reduced infant obstructive apneas.(16,17) It has been estimated that more than one half of the families in the United States practice bed sharing with infants for some period of time.(17)
Death by overlaying is a form of mechanical asphyxia. The entity is ancient, with recordings dating as early as the biblical Old Testament, First Book of Kings, chapter 3, when an infant was "overlain" by its mother and found dead in the bed the following morning. When an infant is overlain by an adult or older child, the infant's airway may be obstructed, the thorax or abdomen may be compressed, or the neck circulation impaired. The autopsy findings in cases of overlaying are usually essentially negative. One may see pressure marks from the bedding or the adult's or older child's clothing. However, pressure marks (unlike contusions) can occur after death. Therefore, the infant and scene need to be thoroughly examined to compare pressure marks on the infant with the bedding or clothing of the bed sharer. The lividity pattern may support the position of the infant as well as show blanching due to pressure from the bed sharer. Because the autopsy findings are usually negative, the differential diagnosis includes sudden infant death syndrome (SIDS), overlaying, and suffocation.(5) A thorough scene investigation with interviews is mandatory. Similar to overlaying, wedging is a form of mechanical asphyxia where the face or thorax is compressed, preventing respiration. Again, the autopsy findings are negative except for possible impressions from the compressing objects.
A problem arises when a case is presented as overlaying or wedging and the child has signs of trauma, such as contusions, abrasions, or facial or ocular petechiae. Do victims of overlaying or wedging present with such physical findings? Is the pressure from overlaying or wedging enough to result in trauma, such as bruises and abrasions? Do physical injuries cause one to exclude these entities as a cause of death? These issues steered this 15-year retrospective study in an attempt to determine the likelihood of such traumatic findings in cases of overlaying, wedging, and other accidental asphyxiation.
MATERIALS AND METHODS
We performed a retrospective review of all pediatric forensic cases referred to the Medical University of South Carolina Forensic Pathology Section/Charleston County Medical Examiners' Office over the 15-year period from January 1985 through December 1999. We looked at all cases in which death was certified as overlaying, as well as cases listed as "undetermined: SIDS versus overlaying." The cases were analyzed as to the age, sex, and race of the victim; manner of death; location/bedding; position of the victim and bed sharer; and whether the bed sharer was known to have ingested drugs or alcohol before sleep. The autopsy findings were reviewed to look for documentation of any injuries such as contusions, abrasions, and facial or ocular petechiae. We also analyzed cases of asphyxia due to wedging and other accidental asphyxiation to see if these infants were bed sharing and if they had any significant autopsy findings.
RESULTS
A total of 32 cases were analyzed. Eleven were classified as asphyxia due to overlaying, 10 as "undetermined: SIDS versus overlaying," and 8 as due to wedging. Three other accidental asphyxia deaths were identified: a 5-month-old black boy suffocated on a plastic bag while sleeping; a 6-month-old white boy suffocated beneath an adult body pillow; a 10-month-old girl hanged herself by a pacifier string.
Of the 21 overlaying or "undetermined: SIDS versus overlaying" victims, 16 were males, 5 were females, 15 were black, and 6 were white. The ages ranged from 6 days to 11 months. Ten deaths occurred in adult beds, six in small or twin beds, four on a sofa, and one in a crib. Two of the adult beds were waterbeds. The victims were bed sharing and potentially overlain by the mother in six cases, the father in two cases, one or both parents in two cases, the grandmother in one case, the sibling(s) in six cases, a young cousin in one case, and the mother and/or sibling in three cases. In 12 of the 21 cases, the infant was sleeping with more than one other individual. The victim in the crib was an infant overlain by an older sibling who also slept in the crib. Only two of the adults admitted to consuming alcohol before sleep.
Documented autopsy findings were analyzed.(Table 1) Examination of the 11 cases designated as overlaying showed one victim with three superficial abrasions of the nose and cheek (0.2-0.5 inch in greatest dimension) and two with a single superficial contusion (face, 0.75 inch and side of the head, 2.5 � 2.0 inch). One infant had a single conjunctival petechia; one had "few" scleral petechiae; one had facial petechiae; and one had pressure marks on the nose and face. When the 10 "undetermined: SIDS versus overlaying" cases were likewise analyzed, similar findings were noted. However, no abrasions were noted on any of these 10 victims. One had a single, small, and superficial contusion on the forehead (1.0 inch); one had a single conjunctival petechia; and one had pressure marks with blanched lividity on the face. No other injuries were noted on the 21 victims.
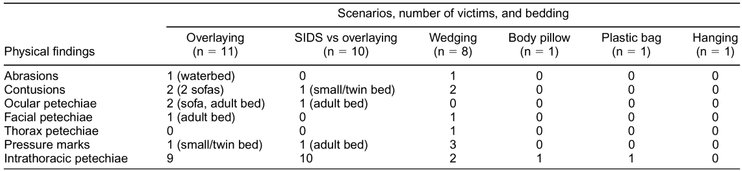
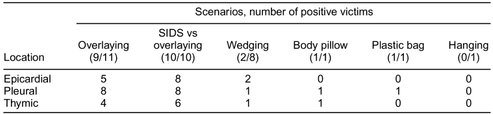
For all cases, the bedding was documented and compared with the presence of physical findings. The one victim with abrasions was sleeping on a waterbed with the mother. The three victims with a single contusion were sleeping on sofas (2 victims, 0.75 inch and 2.5 inches) and a small or twin bed (1 victim, 1.0 inch). The victims with scleral or conjunctival petechiae were sleeping on a sofa (1) and an adult bed (2), while the infant with facial petechiae was sleeping on an adult bed. Pressure marks or blanched lividity were seen on victims sleeping on a small/twin bed (1) and an adult bed (1). Intrathoracic petechiae, often viewed as signs or indicators of asphyxial death, were present in 19 of these victims (9 of the 11 overlaying victims and all 10 of the "undetermined: SIDS versus overlaying" victims). [Table 2]
Of the eight cases of asphyxia due to wedging, the male to female ratio was 3:1, and the black to white ratio was 1:1. The ages ranged from 3 months to 2 years. Two victims were sleeping in their own crib or bed; six were on an adult bed or adult mattress; five were wedged between the mattress and wall; one was between an adult mattress and a piece of furniture, and two were between two adjacent (side by side) mattresses. Only one of the victims was sleeping with an adult or older child. This child was wedged between a mattress and a piece of furniture, and the bed sharer was the father.
The eight wedging victims also had a paucity of physical findings. One victim had a single, small chin abrasion (0.4 inch); two victims had a single contusion (brow, 0.2 inch; cheek, 0.5 inch); one showed facial petechiae; one thoracic petechiae, and three demonstrated linear impressions consistent with the objects of wedging. No oral or intraoral injuries, multiple abrasions, or multiple contusions were identified. Only two of the eight wedging victims showed intrathoracic petechiae, and these two cases were described as "few."
The three additional infant accidental asphyxias were also analyzed. The victim asphyxiated by the body pillow and the victim asphyxiated by the plastic bag showed only rare intrathoracic petechiae, and the hanging victim showed only a neck constriction furrow with no intrathoracic petechiae. No other physical findings, i.e., abrasions, contusions, oral or intraoral injuries, or ocular petechiae, were noted in these three victims.
DISCUSSION
To accurately classify infant deaths that occur during sleep, a thorough history and scene investigation are crucial. The most common cause of death in this group is SIDS. The SIDS autopsy yields negative findings, and the etiology remains unexplained after investigation of the scene and review of the clinical history and medical records. Likewise, homicidal smothering may also have negative autopsy findings, especially in infants.(18) Like SIDS and smothering, overlaying may leave no physical indications as to how the infant died.(19) Autopsy markers of asphyxia may be absent or very subtle in infants.(1,5,6) When an infant is overlain by an adult or older child, several scenarios may occur. The infant's face may be pressed into the bedding, with resultant smothering; pressure on the infant's thorax and abdomen prevent respiration; or, less likely, the neck may be compressed, preventing blood flow to and from the brain.(1,6) With thorax or abdominal compression, the infant's air may be expressed and, lacking the ability to inhale against the pressure, the infant is unable to cry out. These mechanisms of death are speculative because no study can absolutely prove what happens during an overlaying; some individuals even doubt the possibility of such mechanisms leading to death.(18) However, after reviewing 11 reports of bed sharers admitting to finding the infant dead beneath them, the author believes overlaying to be fatal. Some claim that the adult usually consumes drugs or alcohol before sleep, making him or her less likely to be roused by the infant.(12-14) In contrast, in the current study only two adults admitted alcohol consumption before sleep. This similar finding was documented in a recent study by Nakamura et al.(1)
The pattern of livor may help indicate the position of the infant or the pressure points of the overlaying individual. Imprints may also be identified on the infant's skin, recapitulating the fabric pattern of the bedding or the adult's/older child's clothing, supporting the conclusion that the infant was compressed between the bedding and the bed sharer. Any physical signs of overlaying will depend on the size of the bed sharer and the firmness of the opposing surface. For example, the two victims with contusions were on sofas, and the one with an abrasion was on a waterbed, both structures with firm frames when compared to a mattress. Ocular and facial petechiae are also of concern, especially when attempting to rule out strangulation. Others have also reported sofas and waterbeds as particularly dangerous sleeping environments.(5,6,7,13) With neck compression of strangulation, one may see ocular and facial petechiae as venules rupture secondary to the increased pressure as veins are occluded and arterial patency maintained. However, this has been noted to occur less frequently in infants and young children.(18,20-23) In contrast to the neck compression of strangulation, asphyxia by smothering without venous obstruction usually does not present with petechiae, especially in infants.(18,22) In the current 21 overlaying and SIDS versus overlaying cases, only three individuals had ocular petechiae (2 with single petechia and 1 with "rare" petechiae). One victim with a single ocular petechia had facial petechiae.
Wedging occurs when an infant's body or face is compressed within a narrow space, resulting in asphyxia from interference with chest wall movements or obstruction of the airway.(4) Often this compression is between a mattress and a wall, a mattress and a piece of furniture, or between crib slats.(4) Sometimes imprints from the objects the infant was wedged against can be seen on the body, particularly if the object surface was firm.(5) These imprints are usually linear, depicting the border of the bed frame, furniture, mattress, or edge of the wall. Often, there are no physical signs because the pliable skeleton of the infant does not create enough resistance to result in cutaneous or subcutaneous injury. Two of the current cases had a single small contusion, and another had a single small abrasion. Wedging can be a combination of chest and neck compression and thus creates the potential for petechiae, although it is not as commonly seen as in adult wedgings. In one study of infant hanging and wedging deaths, only one of the wedging victims had facial and conjunctival petechiae.(4) The current study found no wedging victims with ocular petechiae and only one case of facial-thoracic petechiae.(4)
Intrathoracic petechiae may be caused by changes in intrathoracic pressure due to forceful respiratory efforts against a mechanical occlusion of the airway.(22) Nineteen of 21 of the current overlaying and SIDS versus overlaying victims had intrathoracic petechiae. Similar upper airway occlusion by the large pillow and the plastic bag also resulted in intrathoracic petechiae in these two victims. Interestingly, only two of the wedging victims showed intrathoracic petechiae, and these were described as "few." No intrathoracic petechiae were seen in the hanged victim. Of note, previous researchers have found few hanged or strangled infants to have intrathoracic petechiae.(9)
Like SIDS victims, overlaying and wedging victims usually have a completely negative autopsy.(6) The presence of intrathoracic petechiae supports the theory of mechanical asphyxia. Intrathoracic petechiae are also present in SIDS victims, but to date the exact etiology and mechanism of death remain unknown.(6) It is the author's opinion that overlaying is a true entity and that unsafe sleeping environments need to be further explored to prevent cases of overlaying and wedging. More importantly, when a child does have positive findings of multiple contusions, abrasions, or oral-intraoral lesions, these probably don't result from overlaying, wedging, or other accidental suffocation. Even in those cases of accidental asphyxia that have an abrasion or contusion, these are usually single, small, and superficial. Furthermore, no oral or intraoral lesions were identified in any of the cases. The pressure required to create such traumatic and often multiple injuries is greater than that pressure from overlaying or wedging. The paucity of physical findings in cases of accidental asphyxia, such as those scenarios described here and reported previously, should impress upon investigators that multiple abrasions, contusions, or oral-intraoral lesions are unlikely to be the result of accidental asphyxia.
REFERENCES
Manuscript received August 21, 2000;
accepted October 15, 2000.
Address correspondence and reprint requests to Kim A. Collins, M.D., Medical University of South Carolina, Department of Pathology, Forensics Section, 165 Ashley Avenue, Charleston, SC 29425, U.S.A.;  Email: Email: Collinsk@musc.edu
Email: Email: Collinsk@musc.edu

Email Charly at: c-d-miller@neb.rr.com