
of Exercise Restraint |
 |
 |
AUTHORS: W. Ann Maggiore, JD, NREMT-P
& Robert B. Palmer, PhD, NREMT-P
Published in the Journal of Emergency Medical Services (JEMS)
March 2002, Vol. 27 No. 3, pages 84-104.
Excerpts from "Exercise Restraint" are posted in NAVY BLUE text.
This article's biggest problem is one that faces ANYONE writing an article about this subject: You simply cannot adequately provide information about more than ONE patient restraint issue in any SINGLE patient restraint article.
Merely to cover the Restraint Asphyxia dangers of restraint requires a 3-part article. Adequate coverage of "legal" issues regarding restraint requires at least a 2-part article! (Part 1 of my 3-Part All Tied Up & No Place To Go article contains MY inadequate coverage of "legal" restraint issues.)
By seeking to cover both "Medical & Legal Issues" regarding restraint in one article, the authors were doomed to failure long before "Exercise Restraint" reached publication.
I'm not an attorney – don't play one on TV; didn't stay at a Holiday Inn Express last night. But, I believe that W. Ann Maggiore presented accurate "legal" issue information.
Unfortunately, her information was limited to merely "introducing" a few of the legal problems associated with inadequate or inappropriate restraint provision. The article entirely failed to specifically describe HOW emergency care providers can avoid legal difficulties related to patient restraint.
Instead of wasting space "justifying" the article's publication by summarizing several studies that identify how emergency care providers are uneducated when it comes to restraint, and how development of PROTOCOLS for safe and effective restraint techniques is grossly neglected – instead of wasting space "justifying" the article's publication with "Examples of circumstances that led to lawsuits" – I'd MUCH rather have read something ABOUT "how to handle violent situations without exposing yourself to unreasonable legal liability!"
Subjecting a patient with decision-making capacity to physical or chemical restraints may leave you open to lawsuits for assault, battery and false imprisonment, as well as medical negligence." Ok. So, HOW do I determine an individual's decision-making capacity without subjecting myself to lawsuits for assault, battery and false imprisonment, as well as medical negligence?!
"To defend against the legal challenges that frequently arise, the [restraint] protocol must call for detailed documentation of the reasons for restraint application, the methods employed and the monitoring of restrained patients." Yeah! So? What ARE the details that we should document? Gosh. They're not offered in this article.
There are plenty other examples of restraint medicolegal issues that were "introduced" in this article, yet never explained. But, I'll stop citing them!
W. Ann Maggiore is an accomplished EMS attorney and care provider. I dearly would appreciate her writing a 2- to 3-part article ONLY about the medicolegal aspects of patient restraint, and EXPLAINING how we can avoid setting ourselves up for litigation! If no hoity-toity hard-copy magazine (such as JEMS) will publish it: I'll post it HERE ... MERGINET.com would post it ... EMSVillage.com would post it! Tons of On-Line EMS and Fire and Law Enforcement "Webzines" would post it.
Yo, Winnie! If you WRITE it, it WILL be posted!

I can't spend much more time on this silly, inadequate article. So, here comes a quickie "summary" of its other inadequacies:
NOT BY ITSELF! It is the combination of agitated or excited delirium AND forceful-prone-restraint that causes death. This article is incredibly inadequate in it's coverage of restraint asphyxia. But, again, ONE article cannot cover the issue.
This article inadequately (even ERRONEOUSLY) addresses physical restraint. And, its focus on chemical restraint is entirely wasted upon the VAST MAJORITY of EMS providers (of ALL certification levels), because FEW of us have the ability to chemically restrain people in the field. Even if we could, we FIRST would have to physically restrain them so that we can get an IV initiated ... or be able to bare their BUTT for an IM injection. Consequently, safe and effective PHYSICAL restraint directions are the first – most important – requirements of any restraint protocol. None were adequately provided by this article.
Plz see the "Why Is 'HAVE THE POLICE RESTRAIN THEM' Entirely Inappropriate and Inadequate to ALL "PATIENT RESTRAINT PROTOCOLS" section of my Web Site's PATIENT RESTRAINT PROTOCOLS Directory. [Figure 8] |
|
|
AH! A QUICK REVIEW OF THE PHOTOGRAPHY!
 [Figure 2] |
|
I am truly thankful for that fact!!! Unfortunately, that's the ONLY safe and effective restraint technique demonstrated by ANY of the photography that accompanies this article. |
[As soon as I finish this long-overdue review and get BACK to the new restraint program slides I'm supposed to be working on right now, I'll be using images from this article to DEMONSTRATE "Ineffective And Dangerous" methods of restraint!]
The "Upper Body" restraint strap is ineffectively and DANGEROUSLY positioned. I think there's an ineffective "hip" restraint strap running across this poor guy's GENITALS! The "Lower Body" restraint strap is ridiculously positioned BELOW the knees. |
|
 [Figure 3] |
Figure 4 (below) is "RICH!" After providing so many examples of how there are NO "approved protocols" for restraint methods, the authors direct readers to rely upon them.
 Multiple restraint methods exist. Check your department's protocols for approved methods. |
|
HANDCUFFS cause injuries and interfere with medical care. They do not belong in ANY ambulance! The "Lower Body" restraint strap is ridiculously positioned BELOW the knees. |
What part of HEAD INJURY
Ah. The SAME PART that gets spaced-off by ALL the providers who end up being litigated for causing forceful-prone-restraint DEATHS – |
|
 |
 "Once you've restrained and adequately sedated an intoxicated individual, place them in the left lateral recumbent position – not prone." |
|
Unfortunately, since the authors have forgotten the fact that CARE must be administered, they are advocating an entirely ineffective "lateral" restraint positioning for a patient in need of thorough examination, assessment, and CARE provision.
SUPINE restraint techniques, |
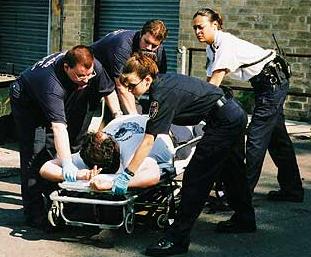
Figure 8 (below) is a wonderful demonstration of how TONS of wasted (dangerous and care-delaying) struggle with someone can occur, when they COULD have been safely and effectively restrained MUCH FASTER, had the restrainers known what the hell to do:
The "Upper Body" restraint strap is ineffectively and DANGEROUSLY positioned.
The arms are ineffectively restrained, and positioned in a manner that will cause headaches should someone actually want to PROVIDE TREATMENT for this individual (like, checking his blood pressure ... starting an IV to get a blood sample, testing it for hypoglycemia ... administering D50 ... etc...) The "Lower Body" restraint strap is ridiculously positioned BELOW the knees. |
|
|
Go Figure.
CONCLUSION
This article is entirely unhelpful in the effort to provide motivation or direction for the creation of safe and effective patient restraint protocols and practices.
I don't "blame" the authors. They knew not what they were doing.

 Email Charly at: c-d-miller@neb.rr.com
Email Charly at: c-d-miller@neb.rr.com